Deformation, Longitudinal Shortening, and Accordion of an Ion Stent
by
Cindy Grines
February 13, 2012Operator(s)
Antwon D. Robinson, M.D., Theodore L. Schreiber, M.D., and Cindy L. Grines, M.D.
Affiliation
Detroit Medical Central Cardiovascular Institute, Wayne State University, Detroit, Michigan
Facility / Institute
Detroit Medical Central Cardiovascular Institute, Wayne State University, Detroit, Michigan
Clinical History
A 65-year-old male with a history of hypertension, hyperlipidemia, diabetes mellitus, cerebral vascular accident complicated by residual left-sided weakness, and status post carotid artery endarterectomy presented to the cardiac catheterization lab with significant angina and positive stress test.
Angiography
Initial angiography revealed an ejection fraction of 65% and the left main, left anterior descending, and left circumflex arteries all with only mild disease. The right coronary artery (RCA) was noted to be a large caliber, dominant, tortuous, moderately calcified vessel with areas of moderate to severe stenoses (proximal 60%, proximal to mid long 80%, and distal 30–40% stenoses).
Procedure
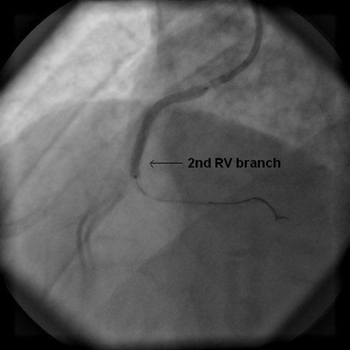
At this time, we decided to intervene on the proximal to mid RCA. A hockey stick – 1 guide catheter was advanced over a wire under fluoroscopy into the ascending aorta and used to engage the RCA (Figure 1 and Figure 2). Subsequently, we advanced a Kinetix guidewire into the distal RCA. Additionally, a Forte medium support wire was also used as a buddy wire into the distal RCA for additional support and to improve the characteristics of the vessel. We were able to advance a 2.5 × 15 mm Apex compliant balloon into the lesion, which was used for pre-dilatation. Due to a suboptimal balloon result and additional disease (or pseudo lesions) noted, it was decided to stent the vessel. A 2.75 × 38 mm Taxus – Ion drug eluting stent was then attempted to be advanced into the lesion in the proximal to mid RCA, but there was significant difficulty with advancing this device into the lesion due to tortuosity and calcification. Consequently, catheter and wire disengagement was appreciated. Reengagement with the hockey stick – 1 guide catheter was obtained and wires were repositioned distal to the lesion. We were able to slowly and carefully advance the stent with correct deployment under angiography the second time (Figure 3). The stent was deployed at 12 atmospheres. The stent balloon was then deflated and removed, but it was noted that the guide catheter was disengaged a second time along with wire dislodgement. We accordingly attempted to rewire the vessel using multiple wires including whisper and balance middleweight wires, but we were unsuccessful as the wires were snagging on the proximal edge of the stent. We also tried a different guide catheter [Judkins right 4(JR4)]; nevertheless, we were not able to advance a wire beyond the stent.
Conclusion(s) / Result(s)
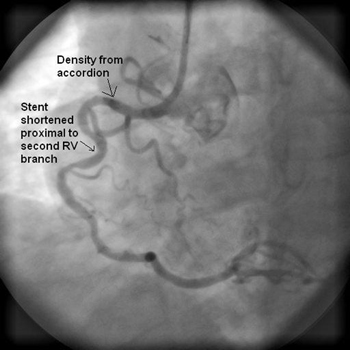
Postintervention angiogram revealed good flow, but there was some mild residual stenosis in the mid portion of the stent. Upon further review of the films, the proximal and distal portions of the stent appeared to be deformed, accordioned, and shortened (Figure 4).
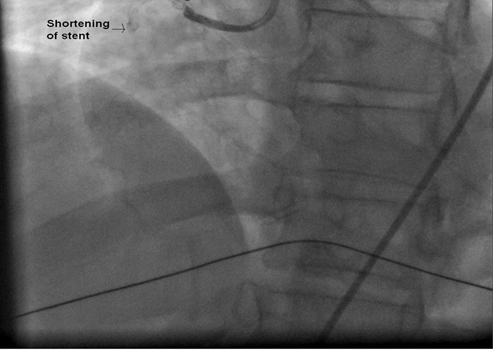
The patient re-presented to the emergency department 5 days later secondary to sudden onset of chest pain, which had started on the morning of presentation. He was found to have an acute inferior myocardial infarction; thus, he was brought to the catheterization emergently. Using a JR4 guide catheter, the RCA was demonstrated to be completely occluded proximally just prior to the stent that was recently placed. Although we attempted for a prolonged period of time using multiple wires, we were not able to advance a wire past the proximal of the stent. The wires appeared to be abutting the proximal stent struts, and the stent thrombosis was ultimately thought to be due to stent deformation and probably malapposition. The vessel remained 100% occluded with TIMI 0 flow, and his AMI was managed medically (Figure 5).
The patient re-presented to the emergency department 5 days later secondary to sudden onset of chest pain, which had started on the morning of presentation. He was found to have an acute inferior myocardial infarction; thus, he was brought to the catheterization emergently. Using a JR4 guide catheter, the RCA was demonstrated to be completely occluded proximally just prior to the stent that was recently placed. Although we attempted for a prolonged period of time using multiple wires, we were not able to advance a wire past the proximal of the stent. The wires appeared to be abutting the proximal stent struts, and the stent thrombosis was ultimately thought to be due to stent deformation and probably malapposition. The vessel remained 100% occluded with TIMI 0 flow, and his AMI was managed medically (Figure 5).
Comments/Lessons
The original purpose of the coronary stent was to reduce restenosis by preventing elastic recoil after percutaneous coronary interventions (PCI). Thus, stents were engineered to have adequate radial strength and precise measurement was routinely reported by the manufacturer, allowing physicians to choose a stent based on radial strength criteria. With early generation slotted tube stent designs, stents were more rigid, and shortening was not observed, thus the concept of measuring longitudinal strength not yet conceived. Stent shortening resulting in geographic miss occurred occasionally after deployment of selfexpanding stents; however, this was thought to be due to characteristics of nitinol material and the inherent difficulty in the stent moving during unsleeving of the device.
Over the past 2 decades of coronary stenting, there has been little notice of balloon expandable stents shortening after deployment in the coronary artery. However, at 2 recent interventional meetings, it was noted that stent shortening or accordioning occurred in some patients who received Boston Scientific (Maple Grove, MN, USA) Taxus Element or Omega stents.(1,2) Furthermore, the Manufacturer and User Facility Device Experience (MAUDE) database between April 2009 and May 2011 registered 358 complaints regarding the Element stent platform, of which 288 complaints provided descriptions allowing further analysis.(3) Stent length change was reported in 14.9%, crimped stent damage in 8.0%, and malapposition in 2.1% of complaints. These complaints described the following stent appearance: “compression, accordion, folded, shortened, wrinkled, concertina” all of which seem to describe a problem with longitudinal strength of the Taxus Element and Omega stent design (both are approved overseas but not in the United States). On April 26, 2011 the Taxus Ion stent (the US marketed version of the Taxus Element)wasFDAapproved and over the summer distributed to catherization laboratories in the United States. To our knowledge, our observation of stent accordion in a tortuous vessel is the first reported in the United States. Upon personal experience handling the stent out of the body and observing its action in models, it became clear to the authors that there are differences in longitudinal strength between different stent designs. This has been further substantiated in exhaustive bench testing.(4)
In our case, we believe that the stent may have been incompletely deployed due to the calcification and tortuosity of the vessel. After deflation of the stent deployment balloon, we believe that the “winged” balloon snagged the distal struts during withdrawal, resulting in distal accordion. The proximal stent became accordioned during attempts to recross the stent with multiple wires and deeply engaging the guide. The resulting stent became shortened, accordioned, and some of the struts were likely impinging on the lumen resulting in the angiographic appearance of residual 30% narrowing. Metal struts impinging on the lumen would dramatically increase the risk of subacute stent thrombosis, and also account for the inability to recross the stent during the initial procedure and during the followup attempted PCI.
This case and bench testing studies demonstrating reduced longitudinal strength should raise concerns regarding the use of the Element, Omega, or Ion stent platforms, particularly in tortuous vessels where the stent may be snagged by the balloon or other adjunctive devices.
This case was previously published in the Journal of Interventional Cardiology.
Over the past 2 decades of coronary stenting, there has been little notice of balloon expandable stents shortening after deployment in the coronary artery. However, at 2 recent interventional meetings, it was noted that stent shortening or accordioning occurred in some patients who received Boston Scientific (Maple Grove, MN, USA) Taxus Element or Omega stents.(1,2) Furthermore, the Manufacturer and User Facility Device Experience (MAUDE) database between April 2009 and May 2011 registered 358 complaints regarding the Element stent platform, of which 288 complaints provided descriptions allowing further analysis.(3) Stent length change was reported in 14.9%, crimped stent damage in 8.0%, and malapposition in 2.1% of complaints. These complaints described the following stent appearance: “compression, accordion, folded, shortened, wrinkled, concertina” all of which seem to describe a problem with longitudinal strength of the Taxus Element and Omega stent design (both are approved overseas but not in the United States). On April 26, 2011 the Taxus Ion stent (the US marketed version of the Taxus Element)wasFDAapproved and over the summer distributed to catherization laboratories in the United States. To our knowledge, our observation of stent accordion in a tortuous vessel is the first reported in the United States. Upon personal experience handling the stent out of the body and observing its action in models, it became clear to the authors that there are differences in longitudinal strength between different stent designs. This has been further substantiated in exhaustive bench testing.(4)
In our case, we believe that the stent may have been incompletely deployed due to the calcification and tortuosity of the vessel. After deflation of the stent deployment balloon, we believe that the “winged” balloon snagged the distal struts during withdrawal, resulting in distal accordion. The proximal stent became accordioned during attempts to recross the stent with multiple wires and deeply engaging the guide. The resulting stent became shortened, accordioned, and some of the struts were likely impinging on the lumen resulting in the angiographic appearance of residual 30% narrowing. Metal struts impinging on the lumen would dramatically increase the risk of subacute stent thrombosis, and also account for the inability to recross the stent during the initial procedure and during the followup attempted PCI.
This case and bench testing studies demonstrating reduced longitudinal strength should raise concerns regarding the use of the Element, Omega, or Ion stent platforms, particularly in tortuous vessels where the stent may be snagged by the balloon or other adjunctive devices.
This case was previously published in the Journal of Interventional Cardiology.
Gallery


Conflicts of Interest
None
Comments