Dissection of Proximal and Middle RCA After Stent Implantation
by
Ortega Marcos
November 19, 2012Operator(s)
Ortega Marcos, MD, Loor Agustin, MD
Affiliation
Dept of Invasive and Interventional Cardiology, Omni Hospital. Guayaquil
Facility / Institute
Omni Hospital, Guayaquil, Ecuador
Clinical History
A 45 year old male, current smoker, with an inferior MI and post-MI angina was admitted for coronary angiography two days after the acute event.
Angiography
LM: Normal
LAD: Normal (Figure 1)
LCX: Normal (Figure 2)
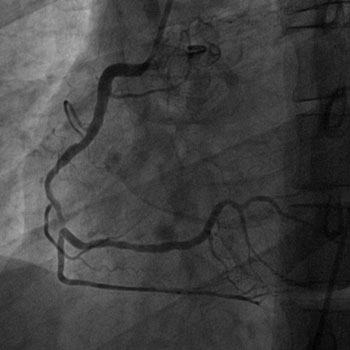
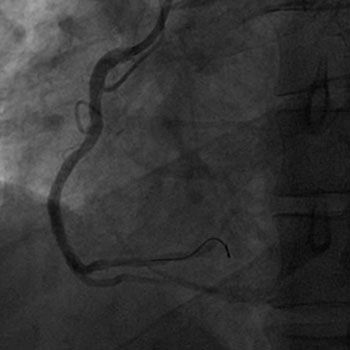
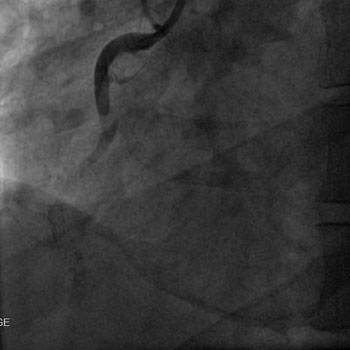
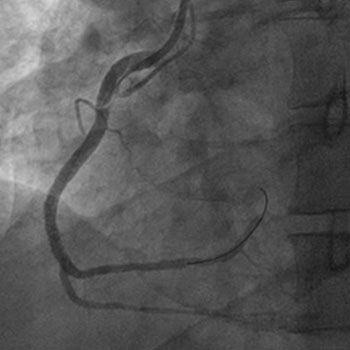
RCA: Sub-occlusion distal (Figure 3)
LAD: Normal (Figure 1)
LCX: Normal (Figure 2)
RCA: Sub-occlusion distal (Figure 3)
Procedure
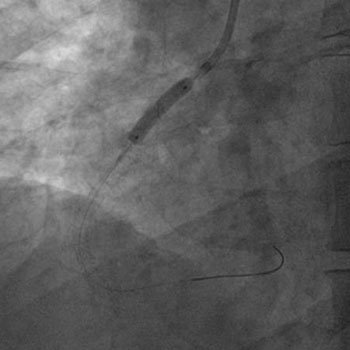
Using a J.R. 4.0 guiding catheter and an ASAHI Fielder FC guidewire, the RCA lesion was pre-dilated with a 2.5x20mm Hopor balloon at 12atm (Figure 4). The distal RCA was stented with a 3.0x18mm Firebird stent at 16atm. The mid RCA was stented with a 3.0x12mm Partner stent at 18atm. Post-dilation was done with a 3.0x12mm balloon at 22atm (Figure 5). The final angiogram showed a Type D dissections and TIMI-0 flow (Figure 6). The patient developed chest pain and hypotension. With great difficulty, other ASAHI Fielder FC guidewire was passed into the distal RCA. The full segment of the mid RCA from the primary stent up to the proximal RCA was stented with four BMS (Figure 7 & Figure 8). An excellent result was obtained with immediate restoration of flow (Figure 9) and normalization of hemodynamics.
Conclusion(s) / Result(s)
Patient was transferred to the CCU in a stable state. He was discharged after 3 days.
Comments/Lessons
Type D dissections represent spiral ("barber shop pole") luminal filling defects, frequently with excessive contrast staining of the dissected false lumen. In this case probably vigorous contrast injection associated with a high blood pressure (200/90 mmHg) maintained during the procedure, despite the use of NTG, produced such a dissection. Appropriately sized and shaped catheters to avoid the contrast injection being directed at a plaque and more gentle initial contrast injections are recommended.
Gallery




Conflicts of Interest
None
Comments