Don’t Lose the Wire Proved Again
by
Saidur Rahman Kahn
April 30, 2012Operator(s)
Dr. Saidur Rahman Khan MD
Affiliation
Ibrahim Cardiac Hospital and Research Institute, Dhaka, Bangladesh
Facility / Institute
Ibrahim Cardiac Hospital and Research Institute, Dhaka, Bangladesh
Clinical History
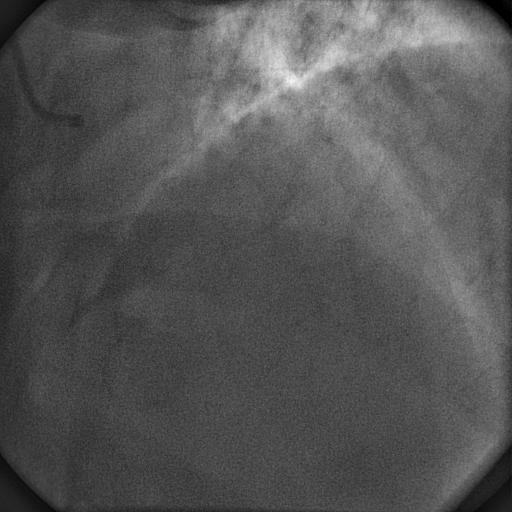
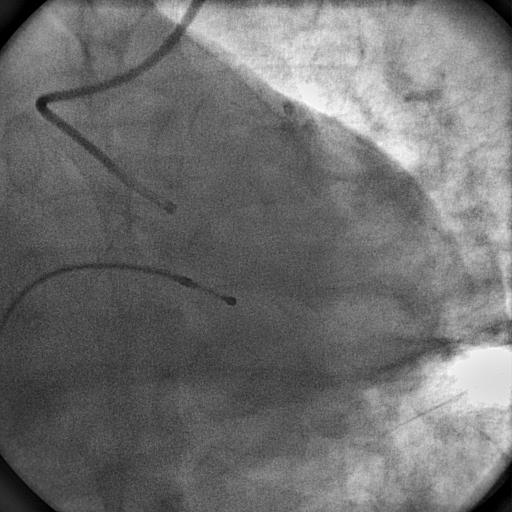
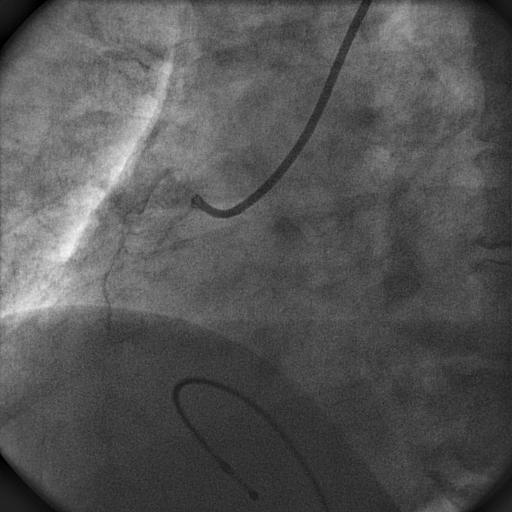
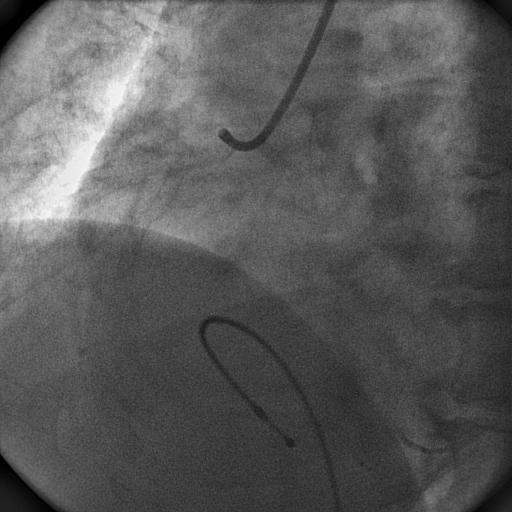
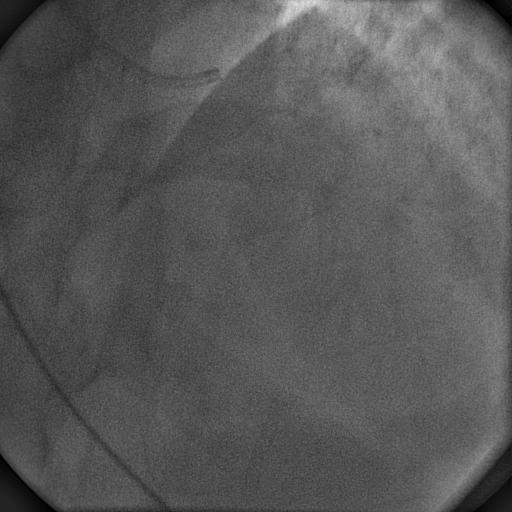
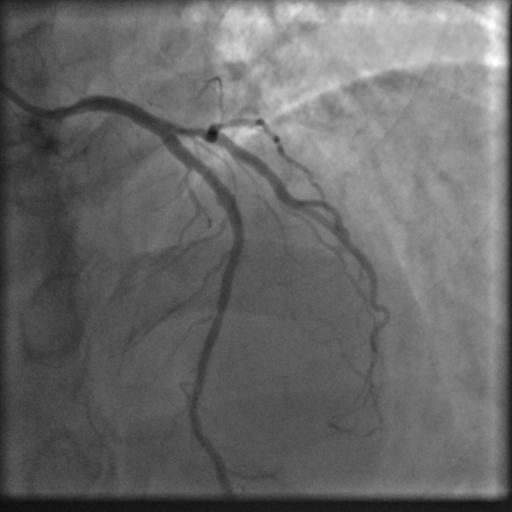
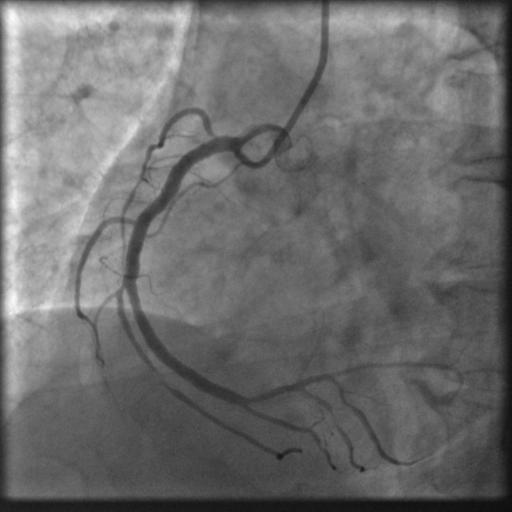
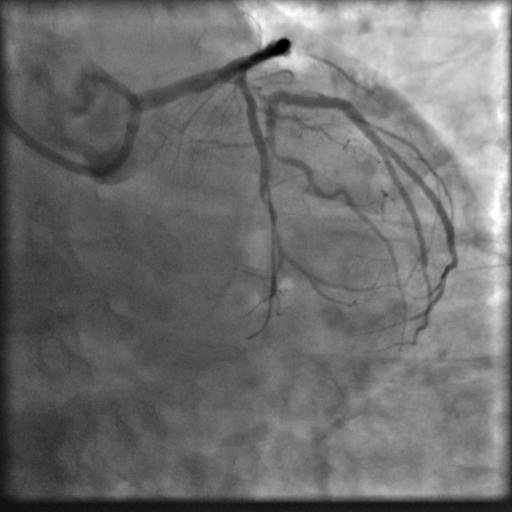
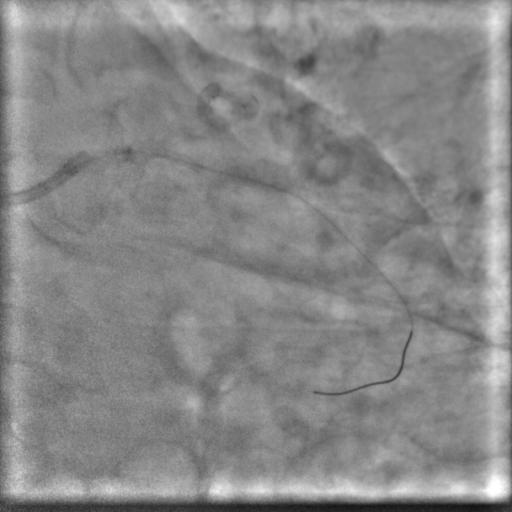
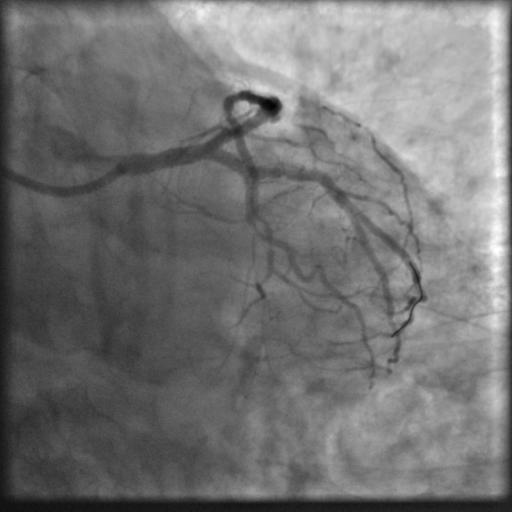
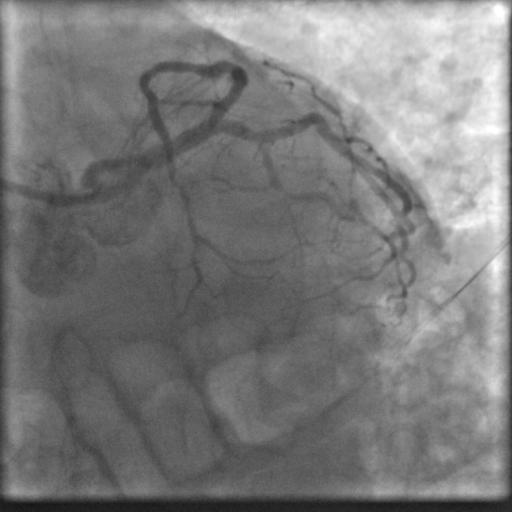
A 55 year old nondiabetic, normotensive gentleman got faint in the morning. ECG revealed ST elevation in inferior and anterolateral leads. The patient was hemodynamically unstable and immediately transferred to the cath lab primary PCI. Door-to-needle time was very brief (less than 90 minutes); and the cath lab procedure started within 2 hours of symptom onset. Angiography, performed by the left transradial approach, revealed severe diffuse triple vessel disease involving the mid LAD (Figure 1), proximal LCX (Figure 2), and totally occluded RCA (Figure 3). A 3.5x28mm CC Flex stent (CoCr) was implanted into the RCA(Figure 4); and the LAD was treated with a 2.5x18mm CC Flex stent distally and a 2.5x23mm EucaTax stent (DES, Eucatech, Germany) proximally (Figure 5). PCI to LCX was deferred because of prolonged procedure time, because the LCX lesion was deemed older, and because total revascularization was not planned as the patient’s hemodynamics and ST segment were dramatically improved after target vessel revascularization. The patient was discharged 4 days after primary PCI. The patient came back 3 weeks after he experienced stable angina (class II).
Angiography
1) Patent stent in LAD (Figure 6)
2) Significant lesion in proximal LCX with severe diffuse disease and a total occlusion of a small caliber distal LCX
3) Patent stent in RCA (Figure 7)
2) Significant lesion in proximal LCX with severe diffuse disease and a total occlusion of a small caliber distal LCX
3) Patent stent in RCA (Figure 7)
Procedure
Using the 6Fr JL 3.0 guiding catheter and a BMW guidewire, the diffusely diseased and totally occluded small calibre distal LCx was wired with 1.25x5mm balloon support and dilated sequentially using the same balloon (Figure 8). The BMW guidewire was pulled back to a large OM branch with the intent to stent the proximal LCX into the proximal OM with a single stent. A 2.5x19mm Taxcor stent (DES, Eurocor, Germany) could not cross and was stuck partly in the left main and proximal LCX. While attempting to withdraw the stent, stent delivery system came out without the stent (Figure 9).Fortunately, the guidewire position was not lost. Despite multiple maneuvers, the stent could not be retrieved. Therefore, we deployed the stent into the distal LMCA and proximal LCX by dilating the dislodged stent gradually and maximally using a 1.25x5mm, 2x15mm, and 3x10mm Sapphire or Sapphire NC balloons.Angiographically it seemed well apposed (Figure 10). Then a 2x9mm Magic Genius (Eurocor, CoCr, Germany) stent was deployed distally to cover the target lesion overlapping it with the previous one. Distal TIMI III flow was achieved (Figure 11). LAD flow was also not compromised.
Conclusion(s) / Result(s)
The patient was discharged 3 days after stenting and was hemodynamically stable.
Comments/Lessons
Sometimes an apparently simple PCI may become complicated and even end up with emergency CABG. The rule “don’t lose the guidewire” can help to salvage a difficult situation. If the wire was not within the dislodged stent, this case would have had a different outcome.
Gallery
Conflicts of Interest
None
Comments