Extensive Intramural Coronary Hematoma Following Balloon Catheter Rupture
by
Francesco Greco
March 19, 2012Operator(s)
F. Greco, R. Caporale, F. Battista, F. Fascetti
Affiliation
SS Annunziata Cosenza, Italy
Facility / Institute
SS Annunziata Cosenza, Italy
Clinical History
A 54 year old male with a history of hypertension was admitted with a diagnosis of NSTEMI: 20 minutes of chest pain, normal ECG, good EF, and minimal increase of Troponin. ASA 300mg, Ccopidogrel 300mg, enoxaparin 0.8ml, and atorvastatin 80mg were started.
Angiography
1) RCA: moderate distal lesions
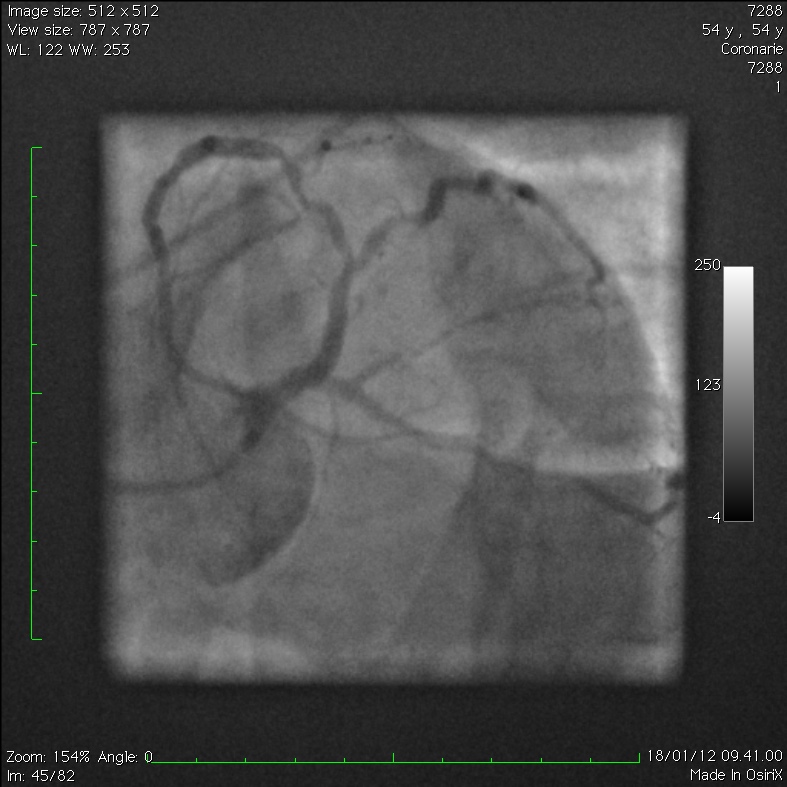
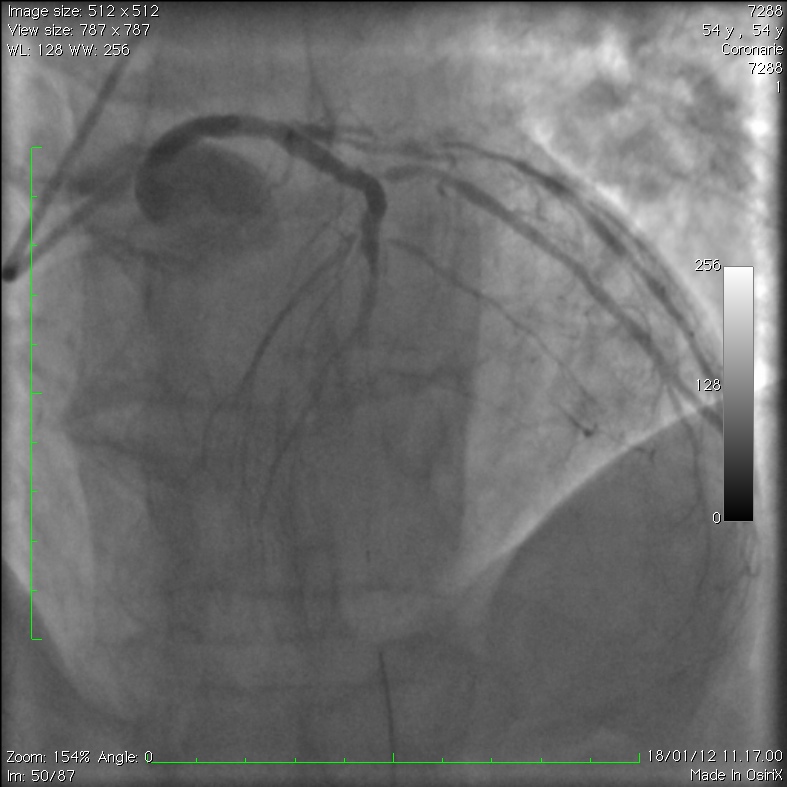
2) LAD: long and severe lesion, moderately calcified, in the mid part involving the first diagonal (Figure 1)
3) LCX: long and severe lesion in the mid part
2) LAD: long and severe lesion, moderately calcified, in the mid part involving the first diagonal (Figure 1)
3) LCX: long and severe lesion in the mid part
Procedure
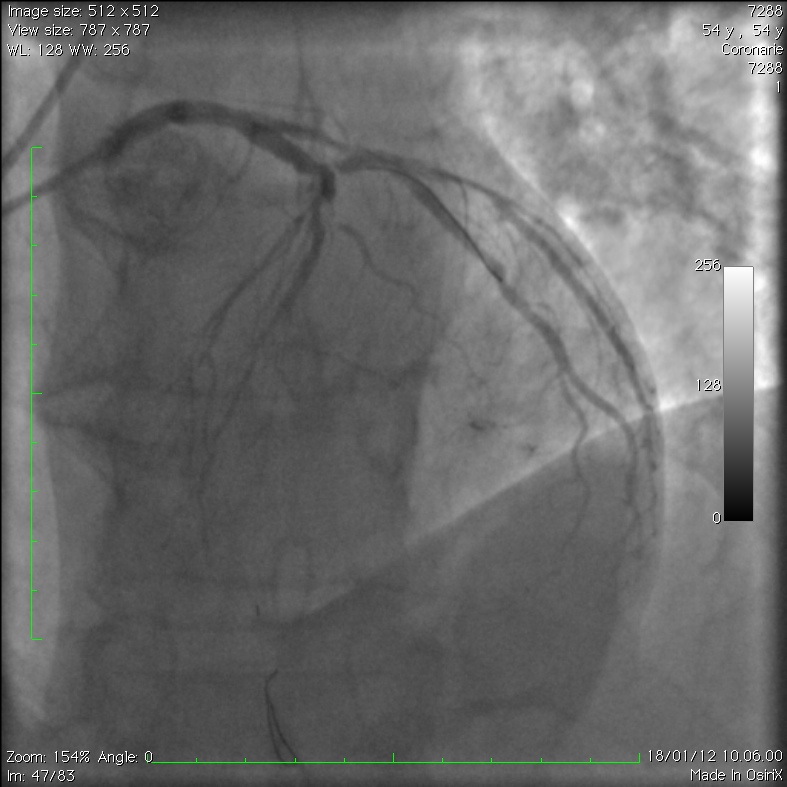
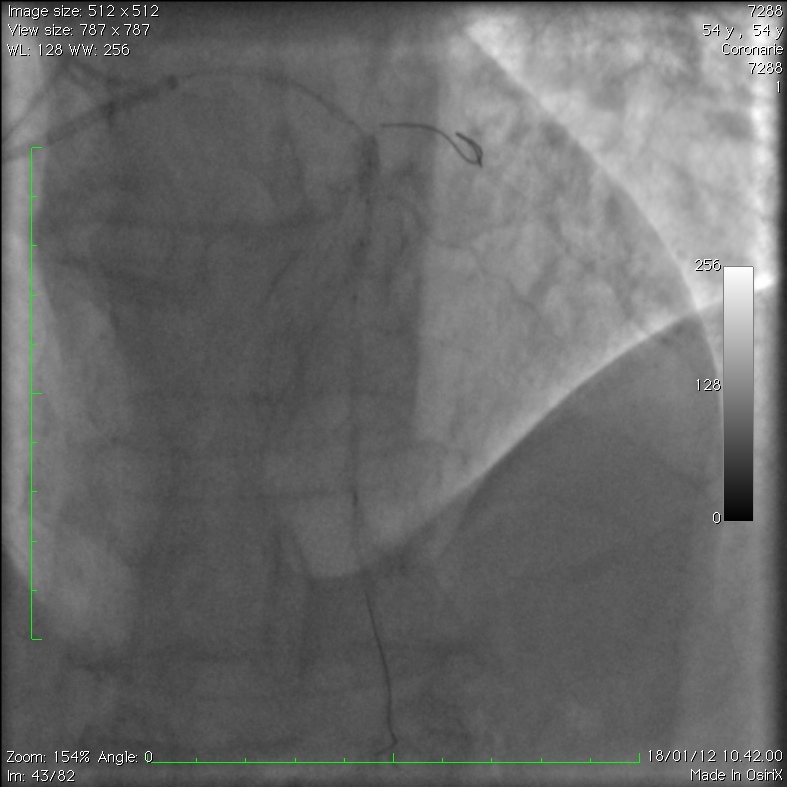
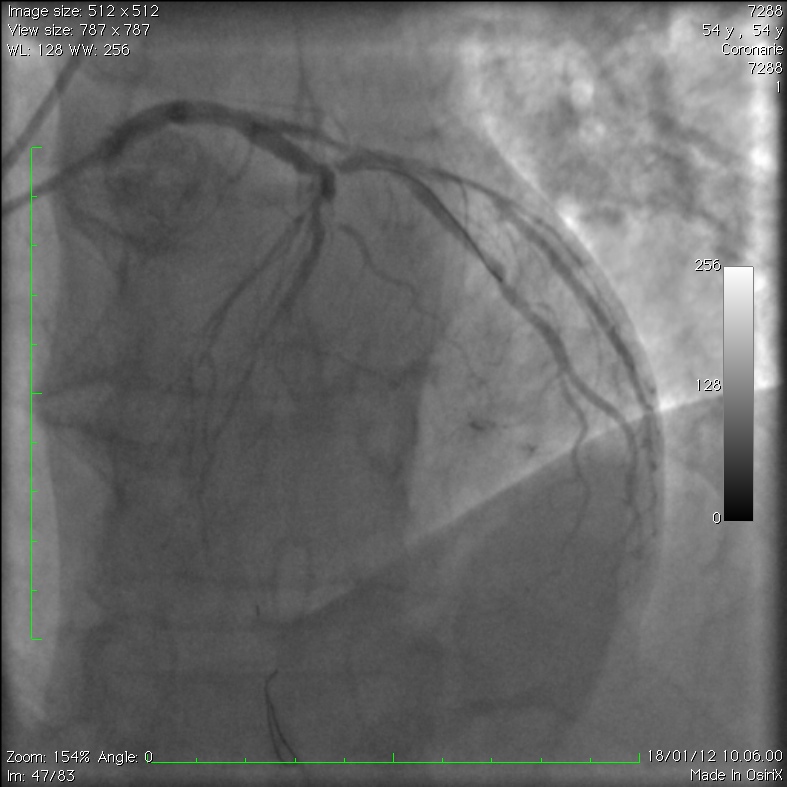
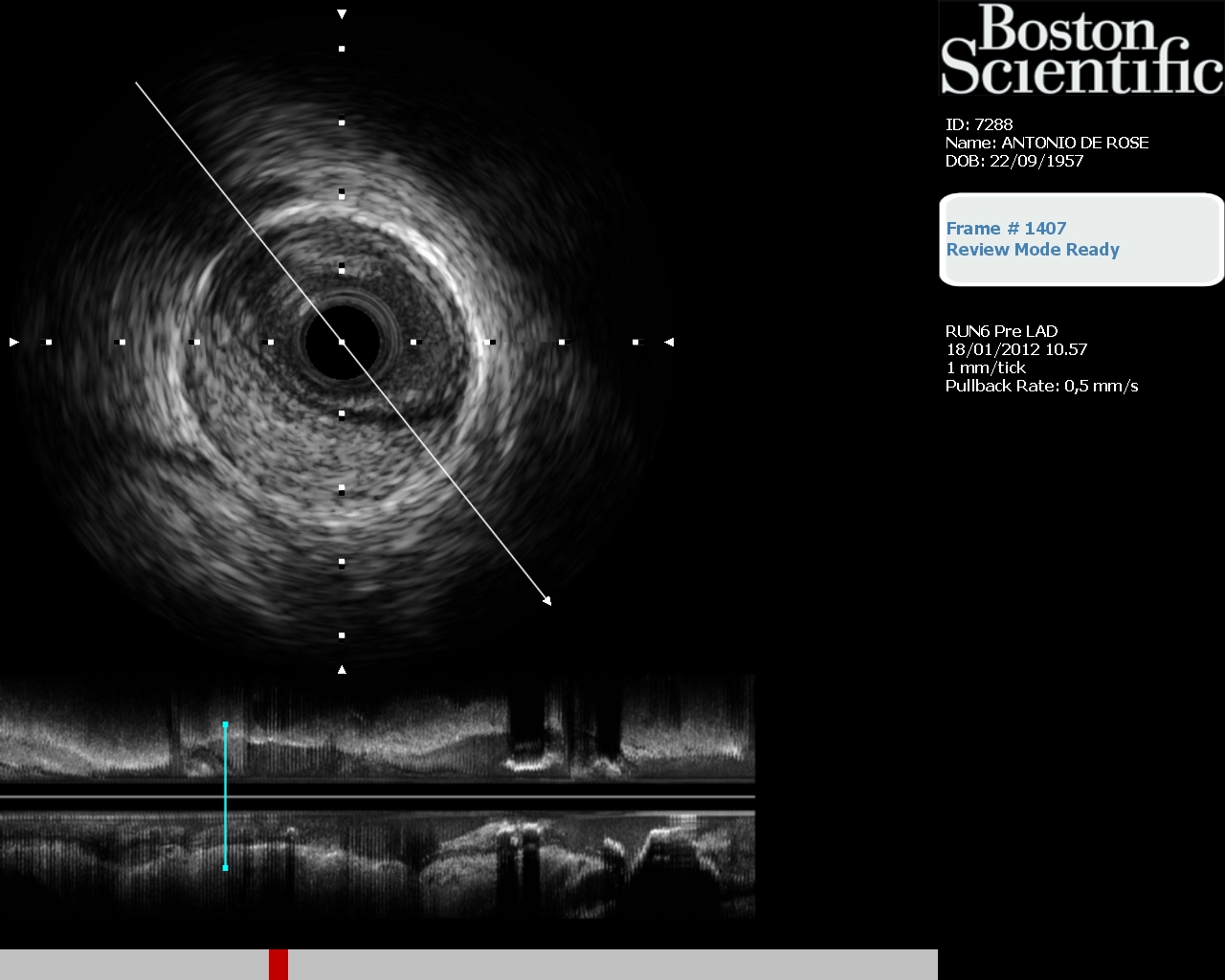
A 6 Fr BL 3.5 (Heartrail III; Terumo) guiding catheter was used to engage the LMCA via the left radial artery. Two BMW Universal (Abbott) guidewires were advanced into the LAD and D1. The mid LAD lesion was predilated with a 2.0x15mm Riujn Plus (Terumo) balloon catheter at 10atm. The second inflation resulted in a sudden decrease of the inflation device pressure with simultaneous appearance of a large amount of contrast media downstream (Figure 2).The balloon catheter was retrieved, and the subsequent image showed flow absence in the LAD down to D1 (Figure 3). The patient was asymptomatic, and the ECG was slightly changed with ST elevation in D1 and AVL. A local administration trough a microcatether (Amicath; IHT Cordynamic) of abciximab 80ml, adenosine 3mg, and nitroprussiate 40 gamma was made without any improvement in coronary flow (Figure 4 and Figure 5). So we performed IVUS of the LAD that showed a large intramural hematoma compressing the true coronary lumen. The hematoma was clearly localized between the adventitia and the media layers and extended from the proximal to the apical segment of the LAD (Figure 6). A BMS stent (Kaname 3.0x28mm; Terumo) was deployed at 14atm in the proximal LAD across D1 to close the entry site of the dissection, without success (Figure 7).
Conclusion(s) / Result(s)
The patient was hemodynamically stable with mild chest pain and was referred to surgery.
Comments/Lessons
a. Unusual modality of balloon rupture: a thin hole, instead a longitudinal cut, resulted in high pressure jet during inflation and full dissection of the LAD
b. IVUS examination was definitive to fully understand the cause and the type of the coronary complication.
c. The best treatment of this type of coronary dissection (intramural hematoma) remains unclear.
b. IVUS examination was definitive to fully understand the cause and the type of the coronary complication.
c. The best treatment of this type of coronary dissection (intramural hematoma) remains unclear.
Gallery

Conflicts of Interest
None
Comments