LM Restenosis Presenting with Acute MI and VF
by
Ahmad Separham
February 27, 2012Operator(s)
Ahmad Separham; Bahram Sohrabi
Facility / Institute
Madani Heart Center, Tabriz University of Medical Science - Tabriz, Iran
Clinical History
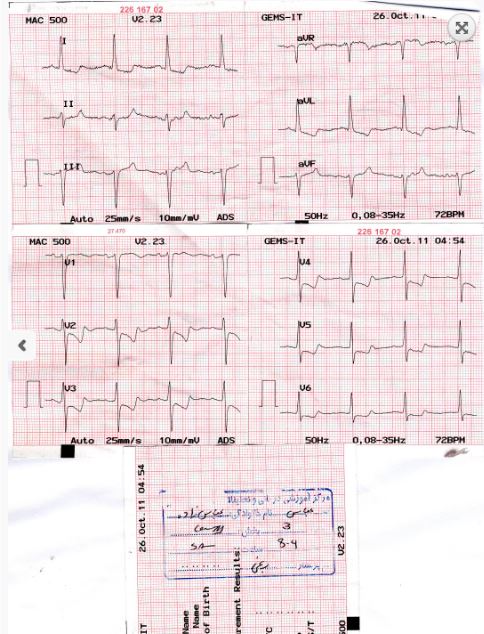
A 59 male patient - with known ESRD, CABG 5 years ago, and implantation of a 3.0x24mm Biomatrix frmo the LM to the LCX 6 months ago - was admitted with ongoing crushing chest pain 3 years ago. ECG showed diffuse ST depression in all precordial leads (figure 1). At initial presentation he developed VF and underwent mechanical ventilation.
Angiography
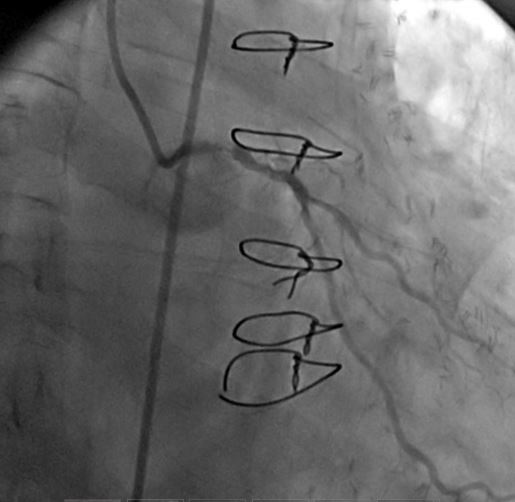
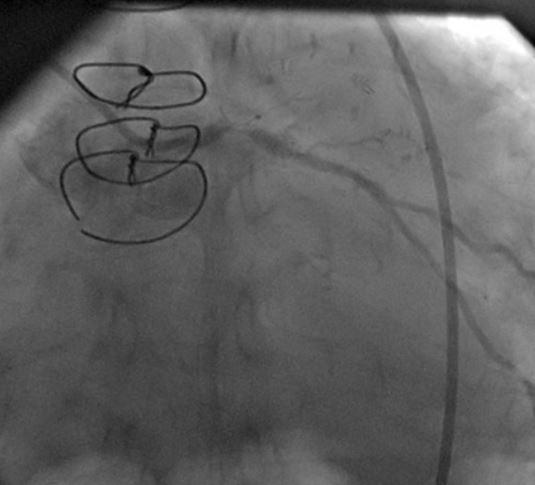
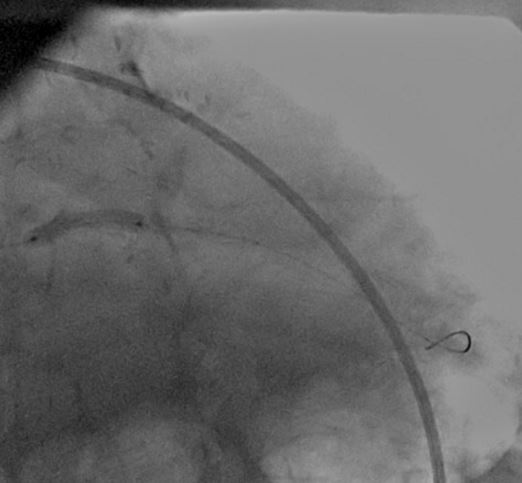
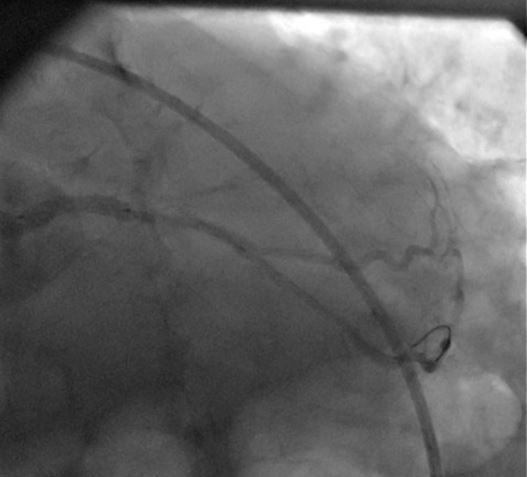
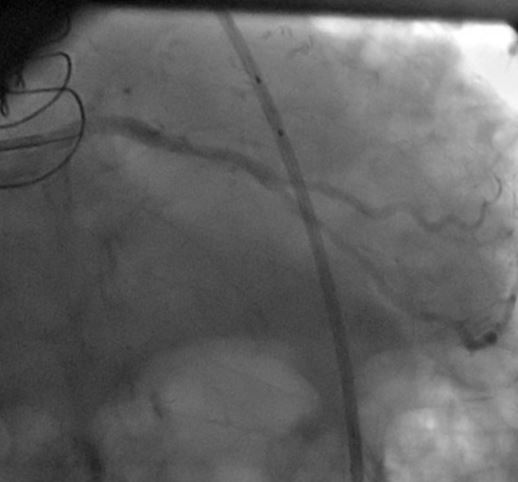
1) LM: subtotal ISR lesion (figure 2, figure 3)
2) LAD: occluded at the ostium and filled via LIMA
3) LCX: proximal non-significant lesion
4) RCA: mild diffuse disease
2) LAD: occluded at the ostium and filled via LIMA
3) LCX: proximal non-significant lesion
4) RCA: mild diffuse disease
Procedure
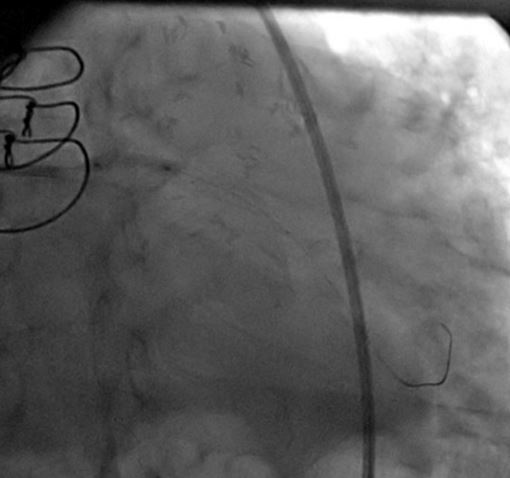
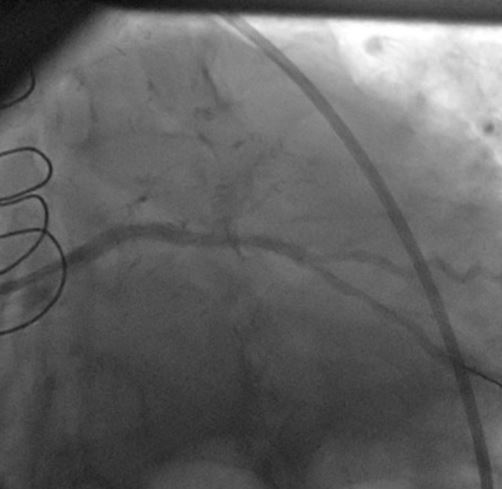
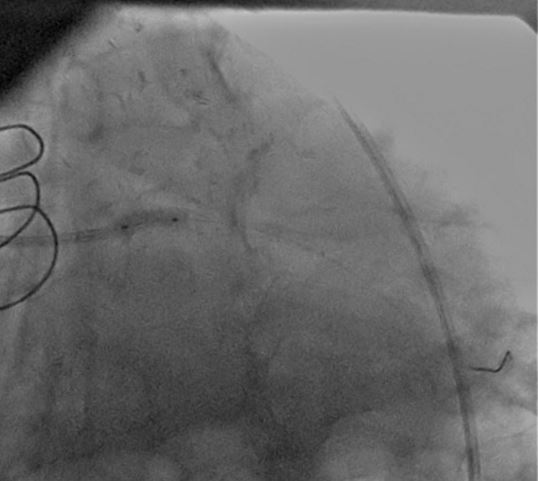
A CLs guiding catheter was used to engage the left coronary artery, and a Choicd floppy guidewire passed through the lesion. The lesion was predilated with a 1.5x15mm and 2x10mm Maveric balloon (figure 4). Then a 3.5x18mm Xience v stent was deployed at 16atm (figure 5, figure 6, figure 7). Post-dilation was done with a 4x10mm Firestar NC balloon (figure 8). The final result showed TIMI-III flow with no residual stenosis (figure 9).
Conclusion(s) / Result(s)
The patient's hemodynamic and respiratory status improved, and he discharged home three days later.
Comments/Lessons
LM restenosis ca present as ACS and even acute myocardial infarction.
Gallery
Conflicts of Interest
None
Comments