LM Stenting in Acute MI with Dissection, Thrombosis, Cardiogenic Shock, and Recurrent Ventricular Tachycardia
by
Sandeep Banga
January 20, 2013Operator(s)
Sandeep Banga MD
Affiliation
St. Stephens Hospital, New Delhi, India
Facility / Institute
St. Stephens Hospital, New Delhi, India
Clinical History
A 27 year old male, occasional tobacco chewer, non-diabetic, and normotensive presented with chest pain of 2 hours duration and was brought to the ER in an unconscious state, pulseless, and with a blood pressure that was not recordable. EKG showed ventricular tachycardia. After DC cardioversion, repeat EKG showed normal sinus rhythm with ST elevation in I, aVl, and V1to V6. Bedside echocardiography revealed an akinetic iinterventricular septum and LV apex and anterolateral wall with an LVEF of 26%. It was decided to do coronary angiography before IABP insertion. During transportation to the Cath Lab, the patient again developed pulseless ventricular tachycardia and was cardioverted; and the blood pressure was still not recordable.
Angiography
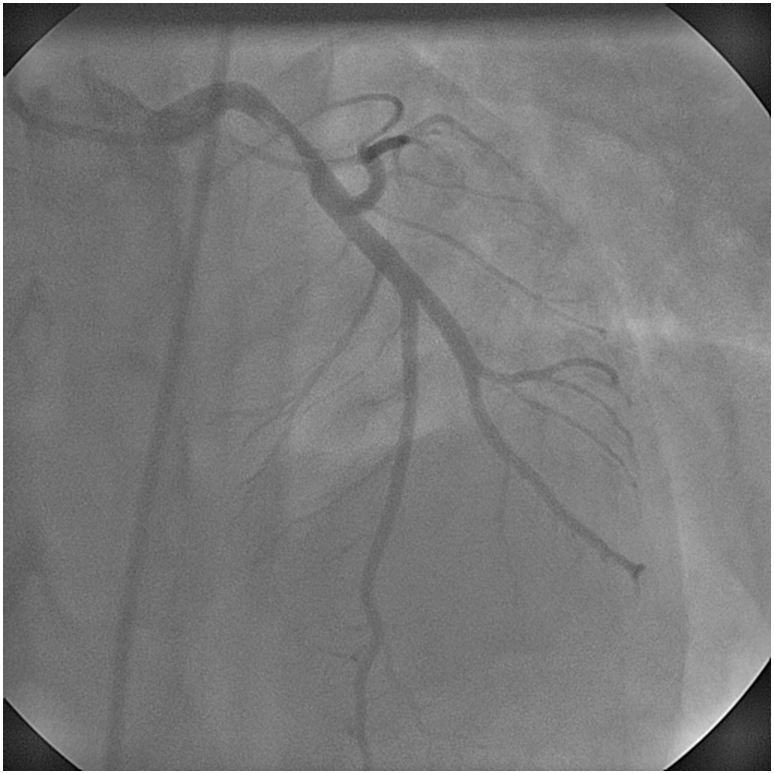
LMCA: large thrombus containing lesion with dissection in mid segment with a 90% stenosis (Figure 1, Figure 2)
LAD: Normal flow (Figure 1)
LCX: Small vessel with normal flow (Figure 1, Figure 2)
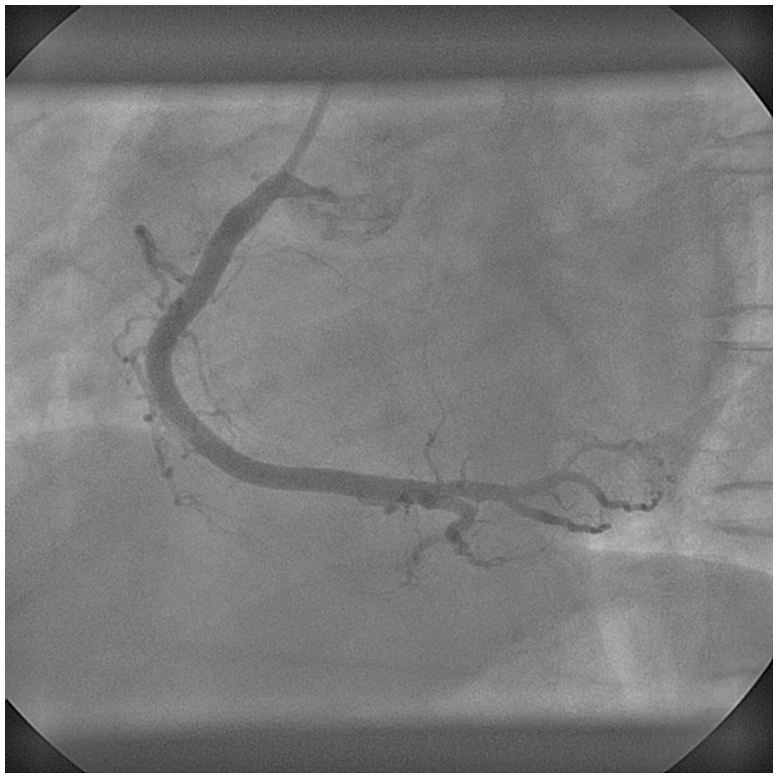
RCA: Dominant and was normal (Figure 3)
LAD: Normal flow (Figure 1)
LCX: Small vessel with normal flow (Figure 1, Figure 2)
RCA: Dominant and was normal (Figure 3)
Procedure
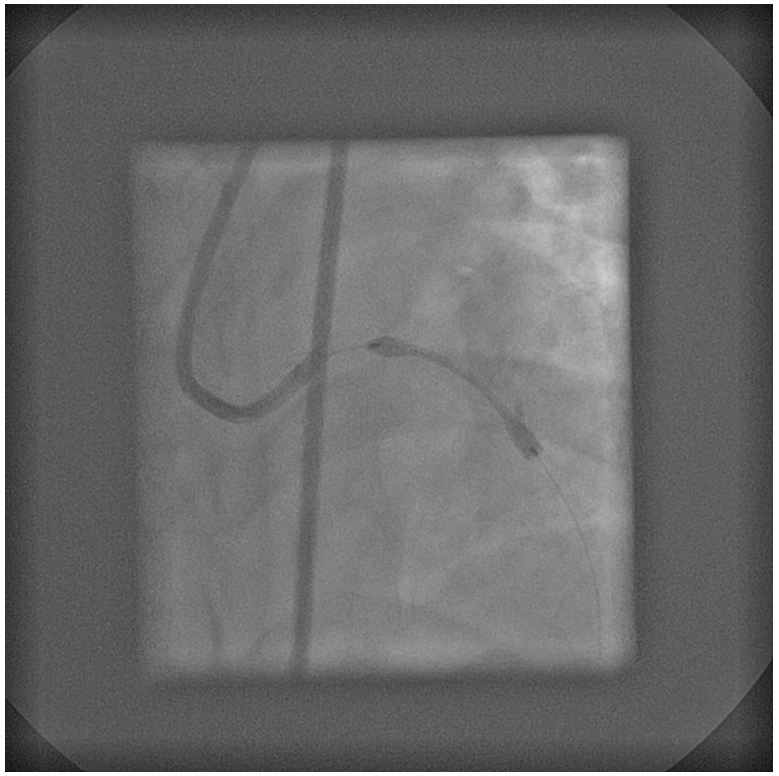
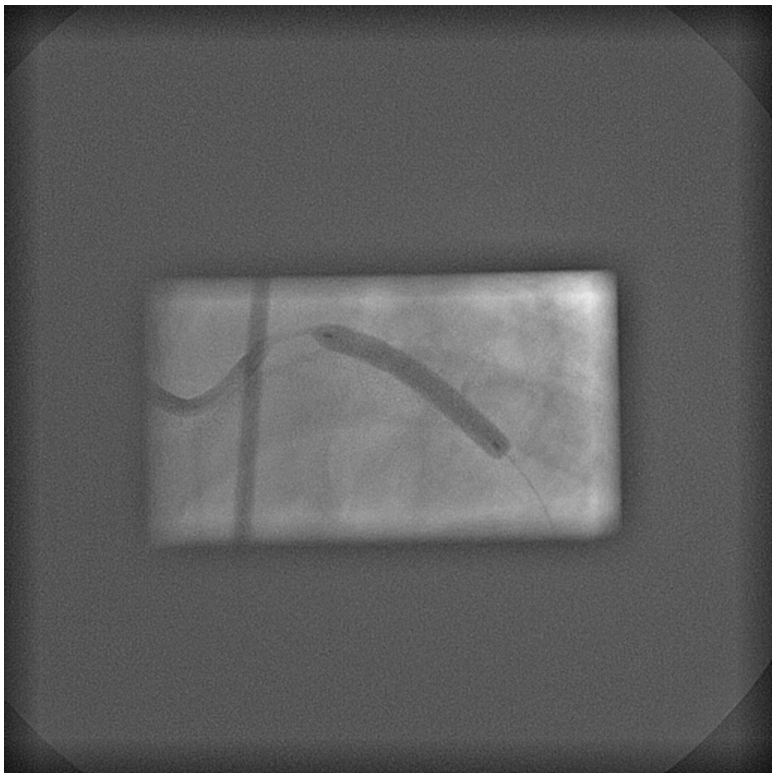
Patient was on inotropic support throughout the procedure, but IABP support was not used during or after the procedure. LMCA was engaged with a EBU 3.5 6Fr guiding catheter. The lesion was crossed using a 0.014” BMW guidewire (Figure 4). The LMCA lesion/dissection/thrombosis was directly stented with a 3.5x25mm Coroflex Please (B Braun Melsungen AG, Germany) stent (Figure 5, Figure 6) at 24atm for 10 seconds; and TIMI 3 flow was restored (Figure 7, Figure 8) with immediate resolution of ST changes. Patient had clinical improvement with blood pressure of 110/70 on the same inotropic supports associated with relief of chest pain.
Conclusion(s) / Result(s)
Patient was shifted to Coronary Care unit in stable condition, and his inotropic supports tapered slowly over 48 hours. He was discharged after 3 days of hospitalization.
Comments/Lessons
Stenting can be done in patients with dissection or thrombosis of the LMCA (or a combination of both pathologies) without IABP support if the patient condition does not allow early CABG or if there is non-availability of early CABG even
if the rest of the arteries are normal. Spontaneous dissection is a rare phenomenon and rarest in the LMCA in males.
if the rest of the arteries are normal. Spontaneous dissection is a rare phenomenon and rarest in the LMCA in males.
Gallery




Conflicts of Interest
None
Comments