Massive Intracoronary Thrombosis Successfully Treated With Multiple Polyethylene Terephthalate Covered Stents
by
Luigi La Vecchia
December 3, 2012Operator(s)
Massive Intracoronary Thrombosis Successfully Treated With Multiple Polyethylene Terephthalate Covered Stents Add to Favorites Add to Favorites Print | 0 By Luigi La Vecchia Monday, December 03, 2012 Operator(s): Luigi LaVecchia, MD
Affiliation
Fellow European Society of Cardiology (ESC), Fellow ANMCO (Associazione Nazionale Medici Cardiologi Ospedalieri), Fellow GISE (Gruppo Italiano Studi Emodinamici), Fellow ACCP (American College Chest Physicians)
Facility / Institute
Bortolo Hospital Viale Rodolfi, Venice, Italy
Clinical History
A 46 year old heavy smoker male patient with a history of mild, untreated hypertension presented with STEMI and was taken to the cath lab for primary PCI. His blood pressure was 90/60mmHg, and his heart rate was 46/min; he was Killip Class I. untreated.
Angiography
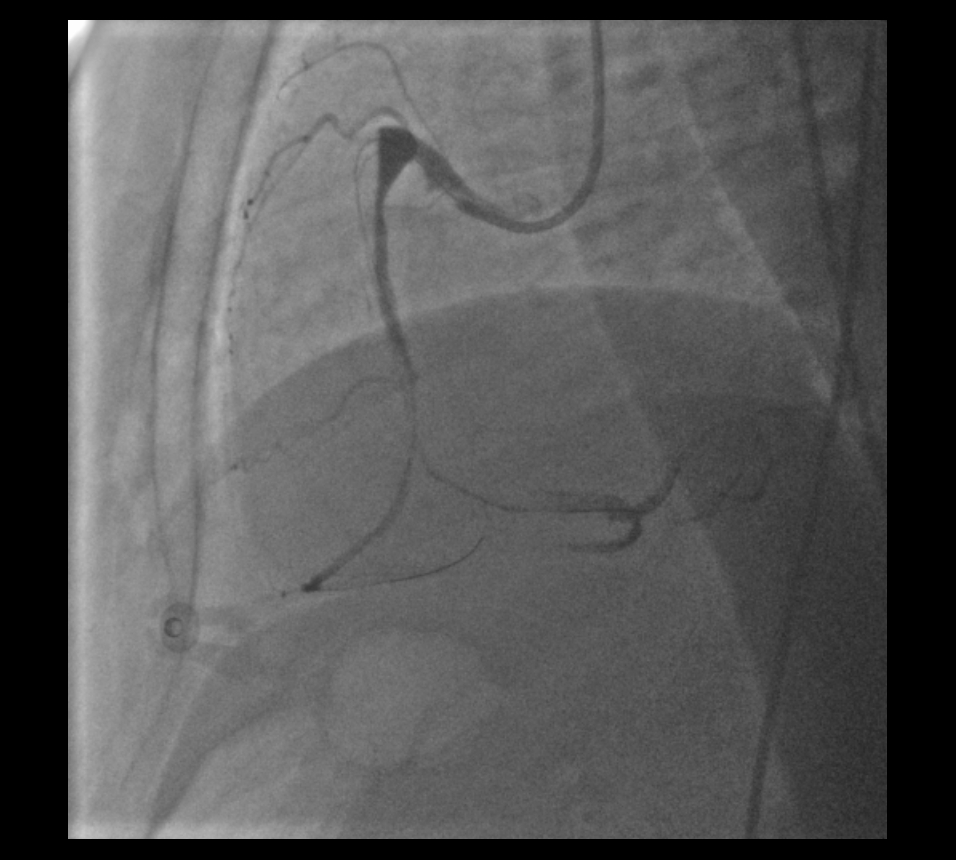
The right coronary artery (RCA) was identified through radial approach by aortography because of a low origin (figure 1). The vessel appeared diffusely ectatic and occluded at mid segment, with evidence of large intracoronary thrombus and minimal distal bed visualization (figure 2). The left coronary artery showed mild ectasia in the proximal segments, especially the left anterior descending (LAD) coronary artery, but was free ofignificant stenoses.
Procedure
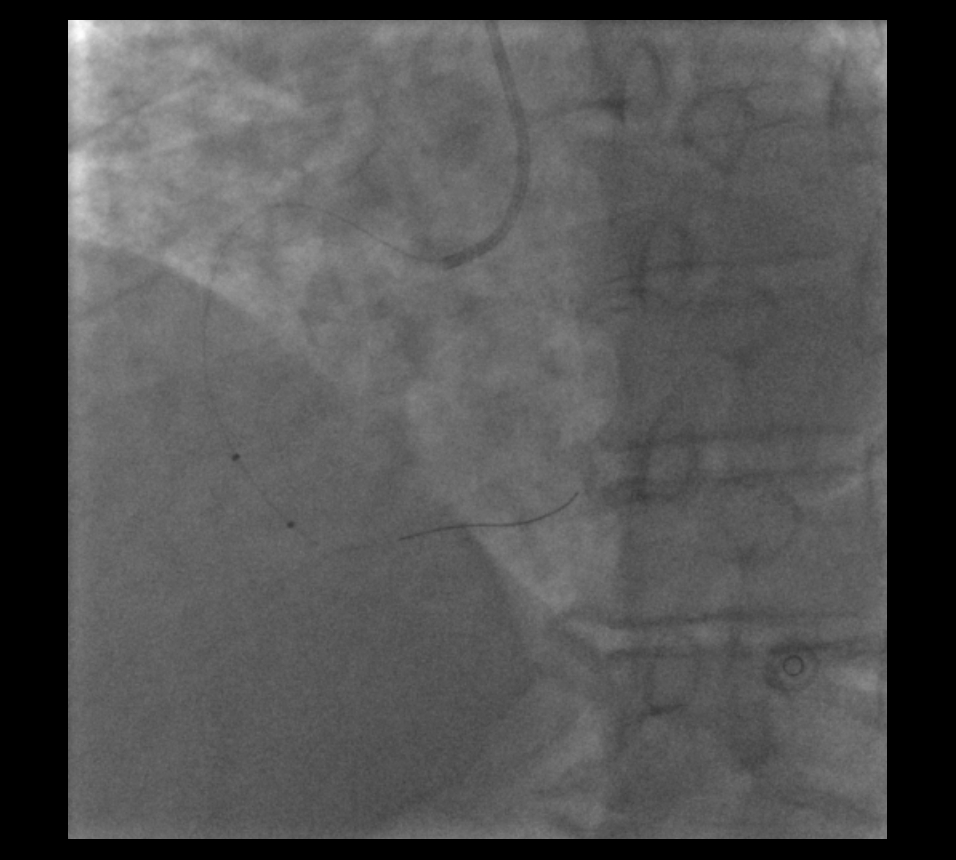
The patient was pre-treated with aspirin and 300mg clopidogrel. Abciximab was used during the procedure along with unfractionated heparin to maintain an ACT of 320s. A BMW universal 0.014" guidewire was positioned in the right marginal branch followed by manual thrombectomy with a Diver CE (Invatec). Despite retrieval of gross material, there was still massive intracoronary thrombus. A second BMW universal 0.014" guidewire was positioned in the distal RCA. Several balloon dilations were performed with Sprinter legend 2.0x15mm and 2.5x25mm balloons without improvement (Figure 3). The guidewire was removed from the right marginal branch, and Angiojet thrombectomy was performed (Figure 4) with minor improvement and a residual massive thrombus. The decision was made to stent the entire segment with Polyethylene Terephthalate (PET)-covered stents (MGUARD, Kardia): 4.0x24mm, 4.0x18mm, and 4.0x15mm. These were all post-dilated with a 4.5x14mm Falcon Grande balloon (Invatec) at 16 to 18 atm. Final result:
Conclusion(s) / Result(s)
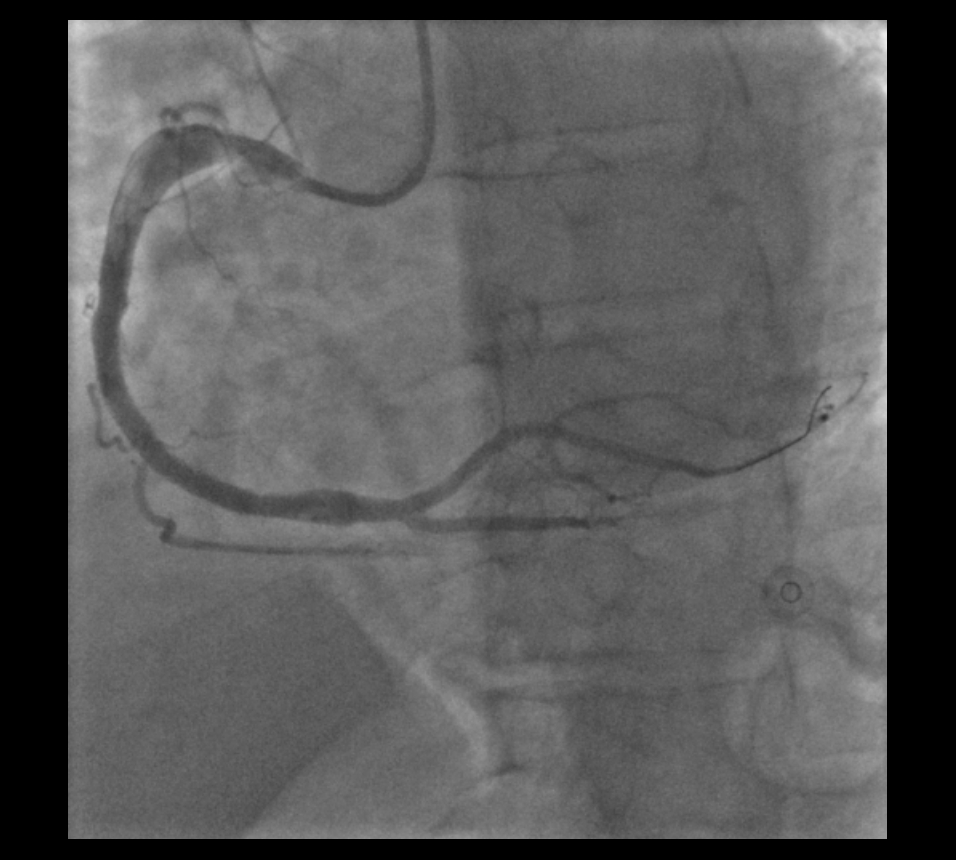
TIMI 3 flow and no angiographic evidence of distal embolization with preserved collaterals (Figure 5).
Comments/Lessons
MGUARD is a valuable option when treating lesions with a high thrombotic burden. Reolytic thrombectomy was only partially effective because of the huge amount of organized material. A distal protection device was an option, but the distal edge of the stented segment was too close to the crux to allow protection for the entire stenting procedure. The MGUARD covered stent provided an excellent result in a high-risk situation.
Gallery
Conflicts of Interest
None
Comments