Protected Distal LMCA Crush Stenting
by
Ayhan Olcay
March 12, 2012Operator(s)
Ayhan Olcay, MD, Kudret Keskin, MD, Fatih Eren, MD
Affiliation
TDV 29 Mayis Hastanesi, Department of Cardiology, Istanbul, Turkey
Facility / Institute
TDV 29 Mayis Hastanesi, Department of Cardiology, Istanbul, Turkey
Clinical History
A 60 year old man had stable angina pectoris for 1 month. He had previos CABG 10 years ago (LIMA-LAD, SVG-RCA). His exercise test was positive. Echocardiography showed inferior hypokinesis, and his EF was 45%. He was non-smoker and on optimal medical therapy.
Angiography
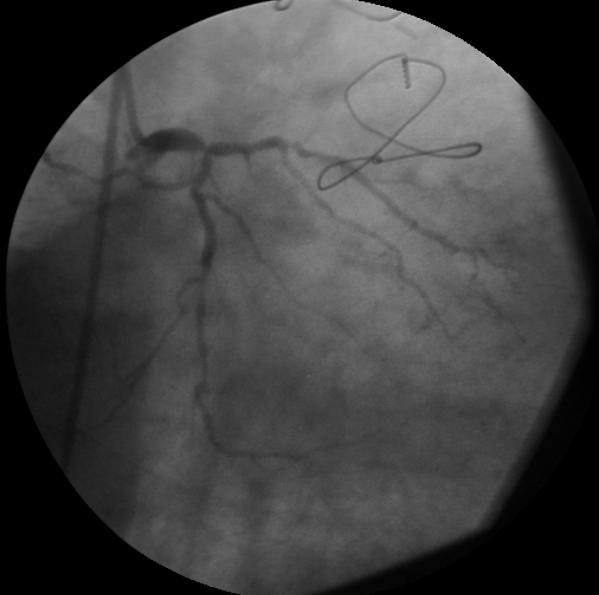
1) LMCA showed subtotal distal occlusion (Figure 1)
2) LAD was occluded from ostium
3) LCX was diffusely diseased and a mid-size ramus branch was seen
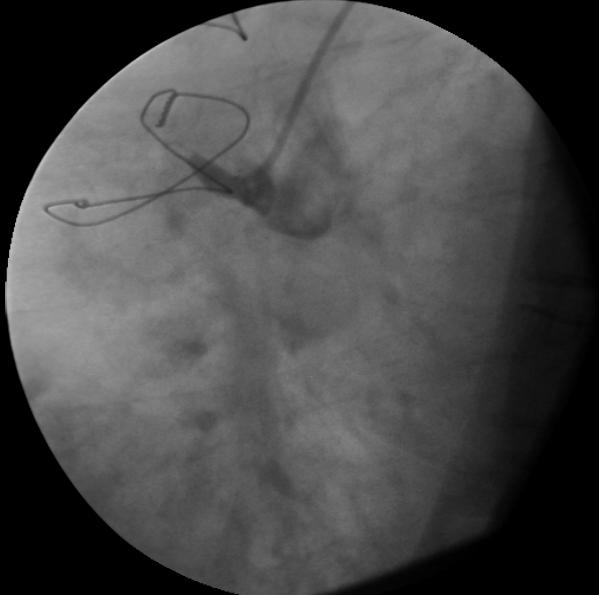
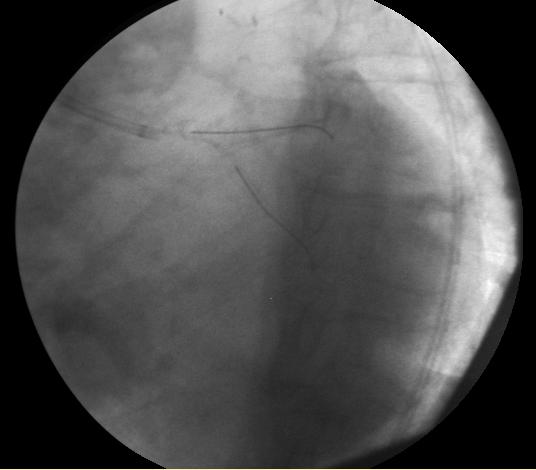
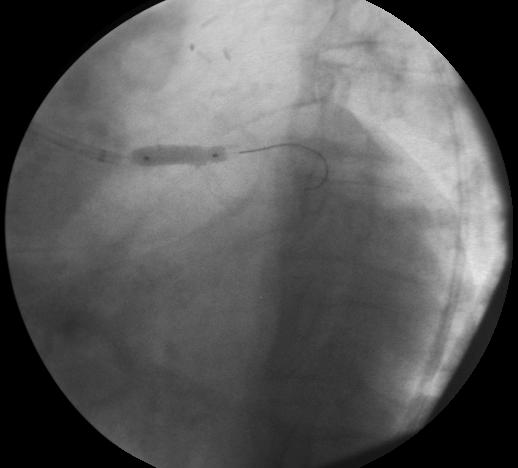
4) RCA was occluded from proximal part (Figure 2).
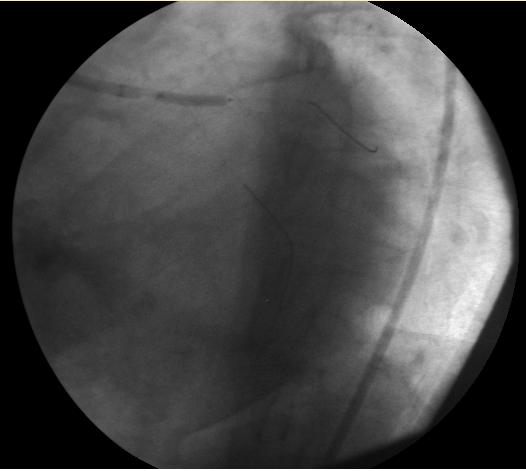
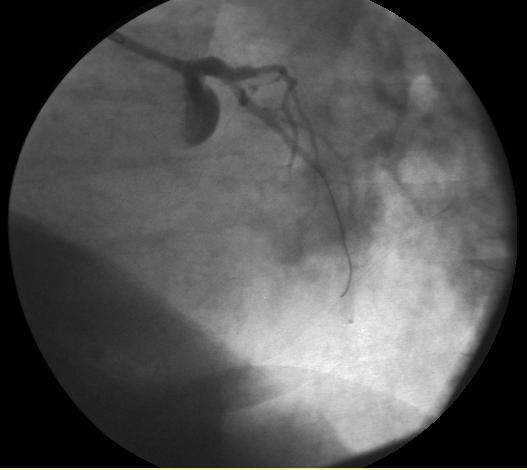
5) SVG-RCA was open (Figure 3).
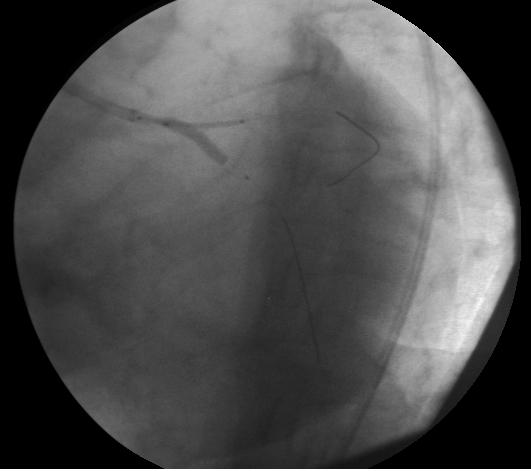
6) LIMA-LAD was open, but the LAD was of small caliber and diffusely diseased (Figure 4).
2) LAD was occluded from ostium
3) LCX was diffusely diseased and a mid-size ramus branch was seen
4) RCA was occluded from proximal part (Figure 2).
5) SVG-RCA was open (Figure 3).
6) LIMA-LAD was open, but the LAD was of small caliber and diffusely diseased (Figure 4).
Procedure
600 mg Clopidogrel, 300 mg Aspirin, Atorvastatin 40 mg, and Heparin 7500 U were given. A 5 Fr sheath was inserted via the left femoral artery in case an IABP was needed. ACT was checked, and heparin administered to have optimal anticoagulation. LMCA was engaged with a 7Fr EBU4 guiding catheter, and floppy guidewires were inserted into the ramus and LCX that were predilated with a Simpass 2.5x15mm balloon (Figure 5, Figure 6). A 2.5x18mm Nobori stent was placed into the LCX, and a Promus Element 3x20mm stent was placed from the LMCA to the ramus. The Nobori stent was withdrawn 3-4mm into the LMCA and inflated at 12atm (Figure 7). The LCX balloon and guidewire were withdrawn, and the ramus stent was inflated at 12atm to crush the stent in the LMCA (Figure 8). When we tried to rewire the LCX with a floppy guidewire, the guidewire kept going under the stent; and the balloon did not follow into the LCX. The stent in the LMCA was post-dilated with a 4x15mm Turquoise balloon for better wall apposition and easier entry into the LCX. The LCX was rewired, and kissing balloon inflations with Simpass 2.5x15mm and Turquoise 4x15mm balloons, both at 10atm, was performed (Figure 9). After kissing balloon inflations and balloon withdrawal, we realized that the ostial part of the LMCA stent was distorted by the guiding catheter (Figure 10). We lost the LCX guidewire position and withdrew the floppy guidwire into the LCX. In order to correct the ostial part of the stent, we inflated a 4.5x15mm Simpass Plus baloon from the LMCA to the ramus at 12atm (Figure 11). Images taken after ballooning showed "orrection"of the stent struts in the LMCA, but the LCX stent showed a new ostial narrowing. Luckily, we rewired the LCX with some difficulty (Figure 12). The LCX ostial struts were postdilated again with a Simpass 2.5x15mm balloon, and the narrowing was corrected (Figure 13, Figure 14).
Conclusion(s) / Result(s)
Patient had mild hypotension and bradycardia during multiple balloon inflations that was corrected by simple volume infusion. There were no EKG changes, troponin elevation, or chest pain at follow-up. Th epatient was discharged next day without any complication.
Comments/Lessons
Crush stent technique requires good apposition of crushed 3 stent layers to the vessel wall and finishing with kissing balloon inflation. While trying to crush a stent, aggressive guiding catheter manipulation may cause stent strut disruption especially in new thin strut stents. Concertina effect (longitudinal stent shortening) is a newly appreciated entity and should be looked for carefully especially with new thin strut stents.
When side branch access is difficult, ballooning proximal part of the main branch provides easier sidebranch access.
When side branch access is difficult, ballooning proximal part of the main branch provides easier sidebranch access.
Gallery







Conflicts of Interest
None
Comments