Treatment of Osteal Cx Stent Restenosis: Need for well rested operator and a winning strategy
by
Ayhan Olcay
June 27, 2014Operator(s)
Ayhan Olcay MD, Vedat Ertunc, MD
Affiliation
Dogan Hastanesi, Department of Cardiology, Istanbul, Turkey
Facility / Institute
Dogan Hastanesi, Department of Cardiology, Istanbul, Turkey
Clinical History
A 66-year-old-man with hypertension and previous stenting to left circumflex (Cx) artery was admitted to our center with a resting chest pain, ST changes in EKG and negative troponin. Transthoracic echocardiography showed normal systolic left ventricular function (LVEF 60%) and normal valvular functions. Patient was stabilized with medical therapy and taken for elective coronary angiography
Angiography
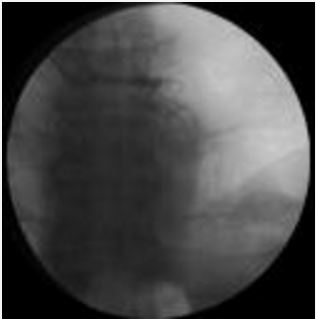
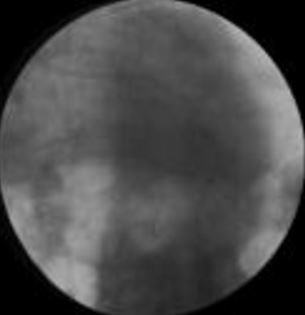
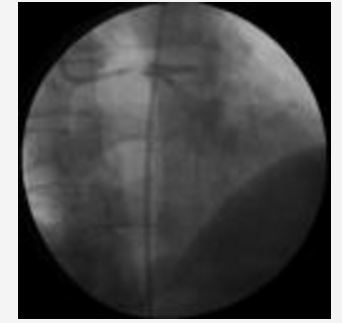
LMCA: Normal without any stenosis (Figure 1).
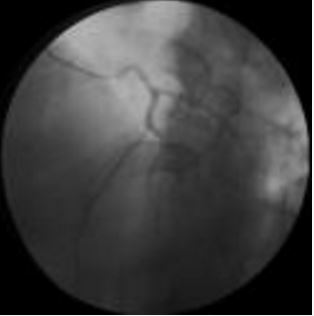
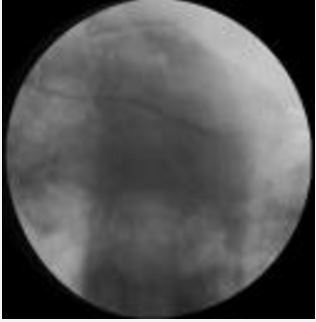
LAD: large vessel with mild osteal and mid level stenosis (Figure 2)
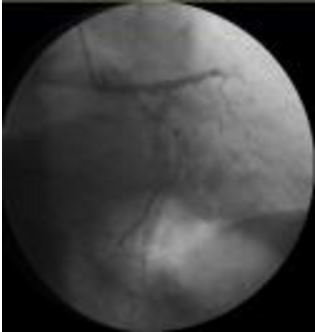
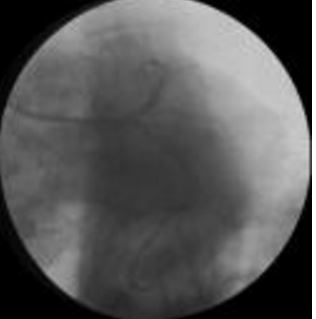
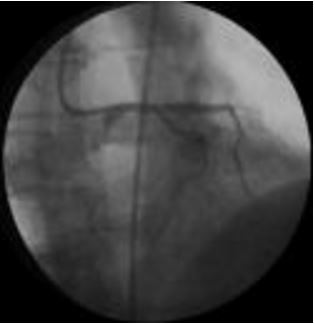
LCX: Severe stenosis within proximal Cx stent (Figure 3).
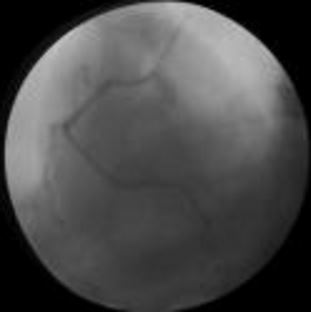
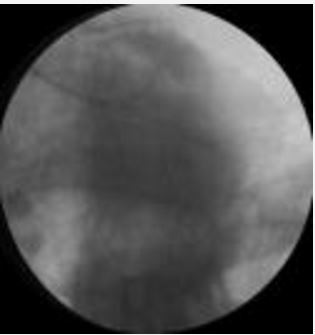
RCA: dominant vessel, with no stenosis (Figure 4)
LAD: large vessel with mild osteal and mid level stenosis (Figure 2)
LCX: Severe stenosis within proximal Cx stent (Figure 3).
RCA: dominant vessel, with no stenosis (Figure 4)
Procedure
The LMCA was engaged with an EBU 4 6 Fr guiding catheter through right radial approach.10000U of heparin was given. An Asahi soft guidewire was placed in Cx and balloon predilatation was made by 2x15 mm RyujinPlus balloon (Figure 5). Before stenting another Asahi soft guidewire was placed in distal LAD. An Orsiro 2.75x26 mm stent was implanted at 12 atm into Cx (Figure 6). Stent was in LMCA by 2 struts. After Cx stenting LAD plaque shifting was observed (Figure 7). A 3x18 mm Orsiro stent was advanced to LAD with difficulty due to the protruding struts of Cx stent. A V-stenting was planned and LAD stent inflated accordingly (Figure 8). During inflation LAD stent balloon ruptured and stent remained unexpanded. Ruptured balloon was removed (Figure 9). Patient was hemodynamically stable without chest pain. At this point primary operator called for help and case was discussed. RyujinPlus 1.5x15 mm and RyujinPlus 2.5x15 mm baloons were passed through unexpanded LAD stent with difficulty and progressively inflated. While a 3.5 mm RyujinPlus balloon was being prepared, LAD wire position was lost and many further attempts proved unsuccessful in rewiring LAD. Operator and team were exhausted, disappointed and case was finished due to long procedure time and high contrast volume (Figure 10). Patient was stable and transferred into CCU. Case was again discussed next morning. Postponing the case for 3 months for stent endothelialization and trying to rewire LAD stent again; trying to rewire LAD stent again in this hospitalization or CABG were the options. We decided to try to rewire LAD stent from femoral route and If successful converting V-stenting into mini-crush in this hospitalization because under-expanded stent in LMCA was a high risk for stent thrombosis. Our strategy was clear this time: Rewiring LAD stent then crushing CX stent by LAD stent and finishing with kissing balloon inflation. LAD was wired after multiple attempts with floppy and Fielder guidewires with different tip shapes (Figure 11). In some successful LAD stent wiring attempts balloon could not pass beyond Cx stent. At the end RyujinPlus 3.5x15 mm NC balloon was passed into LAD stent over Fielder wire. In addition to Fielder wire a floppy wire possibly passing under the struts of LAD stent was left as a buddy wire over which balloon was not advanceable . CX was wired and Cx stent was crushed by 3.5x15 mm RyujinPlus NC balloon in LAD stent (Figure 12). Fielder wire was left in LAD and floppy wire going under LAD stent struts was withdrawn and Cx rewired. Cx ostium was predilated by 1.25x15 mm and 2.75x15 mm RyujinPlus balloons. Case was finished by kissing balloon inflation in Cx (RyujinPlus 2.75x15 mm) and LAD (RyujinPlus 3.5x15 mm) both at 12 atm (figure 13). The result was satisfactory (Figure 14).
Conclusion(s) / Result(s)
The patient was discharged the day after the procedure without any complication by taking 10mg/d prasugrel and 100mg/d aspirin, 40 mg/d atorvastatin, 50 mg/d metoprolol and 5 mg/d ramipril.
Comments/Lessons
Treatment of ostial Cx or LAD lesions require expertise in distal LMCA stenting techniques. Trying to evade distal LMCA stenting techniques invites more trouble. Having a clear planned winning strategy (V-stent, TAP, crush, minicrush) in case a single osteal stent jeopardizes other branch saves alot of time and patient’s life. When operator and catheterization team are tired such high risk cases should be postponed. When a problem is met during intervention being humble and consulting/requesting help of a second operator is very important.
Trying to enter partly deployed LAD stent was not successful with a hook shaped Asahi soft or Fielder guidewires but a simple 45 degree curve from 2 mm tip succeeded to rewire stent. Although it is best to enter a newly deployed stent with a looped wire, trial and error and persistence is sometimes only solution.
We changed initial V stenting strategy plan to mini crash stenting and kissing balloon inflation because we were not sure whether our Cx wire would go within stent lumen or under some struts.
Trying to enter partly deployed LAD stent was not successful with a hook shaped Asahi soft or Fielder guidewires but a simple 45 degree curve from 2 mm tip succeeded to rewire stent. Although it is best to enter a newly deployed stent with a looped wire, trial and error and persistence is sometimes only solution.
We changed initial V stenting strategy plan to mini crash stenting and kissing balloon inflation because we were not sure whether our Cx wire would go within stent lumen or under some struts.
Gallery
Conflicts of Interest
None
Comments