Unprotected LM Stenting in Rapidly Progressive of LM Disease Without the Use of IABP
by
A. M. Thirugnanam
April 23, 2012Operator(s)
A.M.Thirugnanam Sr. Interventional Cardiologist
Affiliation
Kamineni Hospital, Hyderabad, India
Facility / Institute
Ipcard Cardiac Care Center, Musheerabad, Hyderbad, India
Clinical History
A 68 year old female with known hypertension and bilateral knee joint replacement 2 years previously, but no diabetes, had mild CAD treated with medical management. For the last 4 months, she was having CCS-4 angina. ECG showed NSR and nonspecific ST-T changes in all leads. 2D-echo was normal with a left ventricular ejection fraction of 65% and regional wall motion abnormality in the LAD territory. Troponin was negative.
Angiography
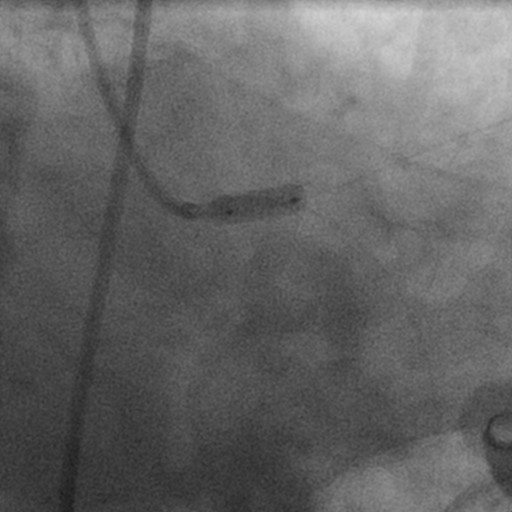
Angiography 6/6/2010:
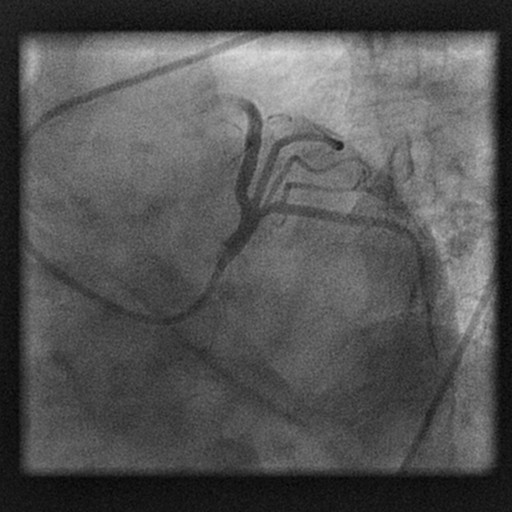
1) LM: mild disease (Figure 1)
2) LAD: proximal mild disease
3) LCX: non dominant and normal
4) RCA: dominant and normal.
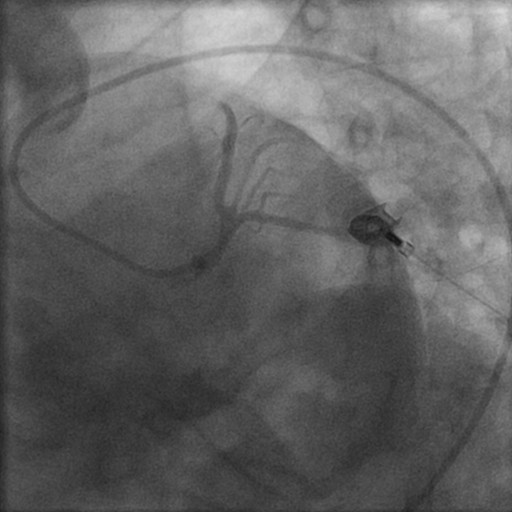
Angiography 1/19/2012:
1) LM: 70% eccentric lesion (Figure 2)
2) Syntax score: 23.
1) LM: mild disease (Figure 1)
2) LAD: proximal mild disease
3) LCX: non dominant and normal
4) RCA: dominant and normal.
Angiography 1/19/2012:
1) LM: 70% eccentric lesion (Figure 2)
2) Syntax score: 23.
Procedure
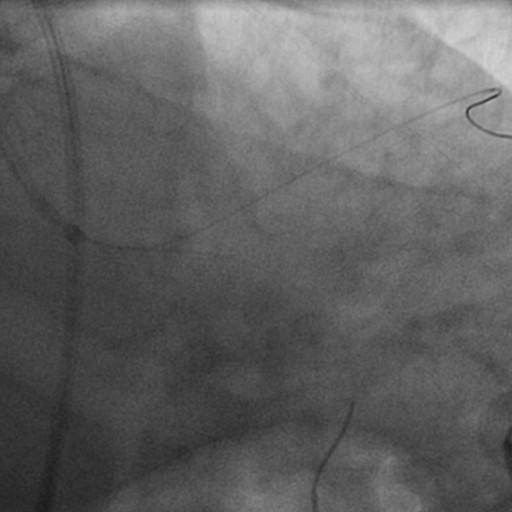
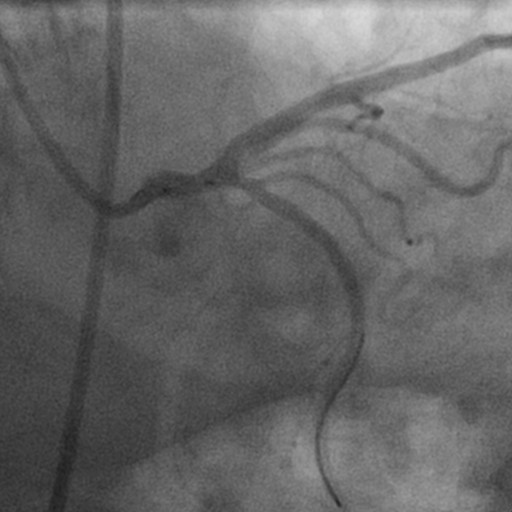
Bivalrudin was given during procedure and after the procedure according to weight along with a loading dose of clopidogrel-600mg, aspirin-325mg, and atorvastatin-80mg. The LM was engaged with a JL-6 Fr guiding catheter through the right femoral approach (Figure 3). Two BMW guidewires were placed in distal LAD and distal LCX (Figure 4). Predilation was performed with a 3x10mm Maveric balloon at 10atm (Figure 5). Finally, a 4x12mm Xience Prime (Abbott) stent was deployed at 14atm with flaring of the ostium using the same stent balloon at 16atm pressure. Final results showed TIMI-3 flow, and no residual dissection (Figure 6).
Conclusion(s) / Result(s)
The patient tolerated the entire procedure and was kept in the ICCU for 2 days.
Comments/Lessons
Very fast progression of LM disease is a major concern in older adults. Recent Syntax results gives confidence regarding unprotected LM stenting with less than 30 Syntax score.
Gallery

Conflicts of Interest
None
Comments