Use of Angiojet in Primary Angioplasty (PCI) of a Giant Right Coronary Artery
by
Than Aung
August 20, 2012Operator(s)
T.H. Aung , Tan K. B Julian, Ooi Y. Wei, Ong J.L. Paul
Affiliation
Department of Cardiology, Tan Tock Seng Hospital, Singapore
Facility / Institute
Department of Cardiology, Tan Tock Seng Hospital, Singapore
Clinical History
1) LMCA: distal 40% lesion.
2) LAD: diffusely atherosclerotic, but unobstructed.
3) LCX: ostial 80% lesion, but there was TIMI 3 flow .
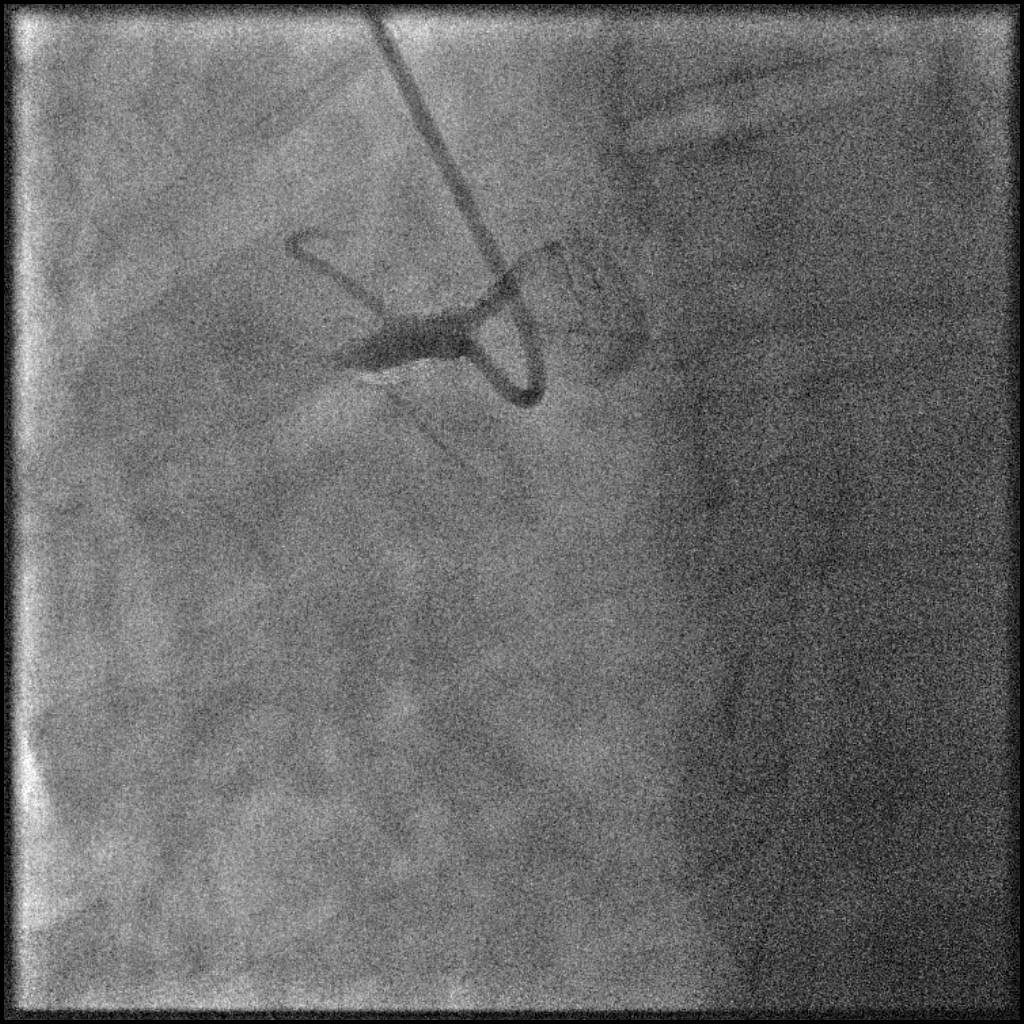
4) RCA: a large vessel and completely occluded proximally soon after the conus branch (Figure 1).
2) LAD: diffusely atherosclerotic, but unobstructed.
3) LCX: ostial 80% lesion, but there was TIMI 3 flow .
4) RCA: a large vessel and completely occluded proximally soon after the conus branch (Figure 1).
Angiography
N/A
Procedure
Procedure:
Primary PCI was done via 6Fr right radial approach. Intra-arterial enoxaparin 0.5mg/kg and 200mcg NTG were was given via the radial sheath.The RCA was difficult to cannulate having tried IL3.5 and JR3.5 guiding catheters. It was eventually intubated with an AL0.75 Cordis guiding catheter. Two boluses of 9mg intra-coronary integrilin were given 10 minutes apart followed by an iv infusion. Four doses of intra coronary adenosine 100mcg were given during the procedure.
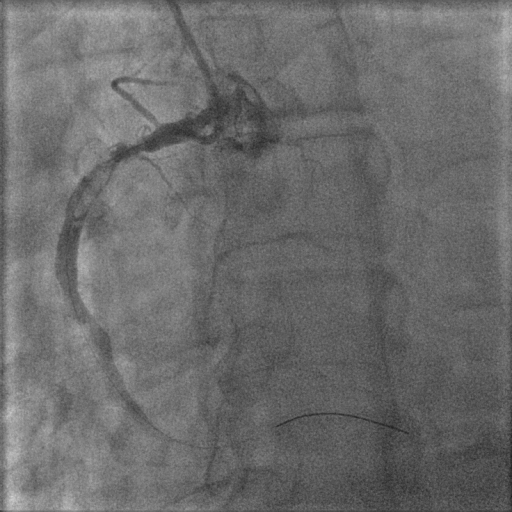
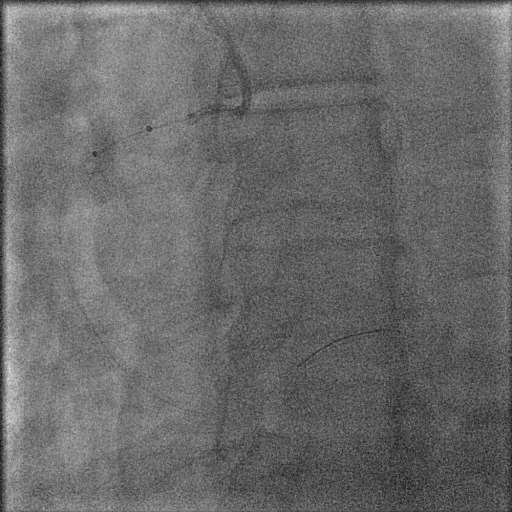
The occluded RCA was crossed with 0.014” Run Through intermediate guidewire (Terumo, Japan). Export AP thrombectomy catheter (Medtronic, USA) was used to remove some of the clot. Post aspiration showed TIMI 2 flow with extensive residual thrombus (grade 4, Figure 2). Further pass of the Export catheter made little impact. The patient went into VF, and he was given 2 DC shocks to restore sinus rhythm. An Angiojet Spiroflex 4Fr (Medrad, USA) with back up transcutaneous pacing was inserted, and 30ml of fluid were removed (Figure 3) to significantly reduced the thrombus burden and restored TIMI 3 flow (Figure 4) reduce ST segment elevation. The vessel was subsequently stented with a 5.0x24mm Liberte bare metal stent (Boston Scientific, USA) at 15atm achieving a good result (Figure 5). There was distal plaque shift which improved somewhat after another run using the Export catheter followed by low pressure dilation with a 5.0x15mm balloon.
Primary PCI was done via 6Fr right radial approach. Intra-arterial enoxaparin 0.5mg/kg and 200mcg NTG were was given via the radial sheath.The RCA was difficult to cannulate having tried IL3.5 and JR3.5 guiding catheters. It was eventually intubated with an AL0.75 Cordis guiding catheter. Two boluses of 9mg intra-coronary integrilin were given 10 minutes apart followed by an iv infusion. Four doses of intra coronary adenosine 100mcg were given during the procedure.
The occluded RCA was crossed with 0.014” Run Through intermediate guidewire (Terumo, Japan). Export AP thrombectomy catheter (Medtronic, USA) was used to remove some of the clot. Post aspiration showed TIMI 2 flow with extensive residual thrombus (grade 4, Figure 2). Further pass of the Export catheter made little impact. The patient went into VF, and he was given 2 DC shocks to restore sinus rhythm. An Angiojet Spiroflex 4Fr (Medrad, USA) with back up transcutaneous pacing was inserted, and 30ml of fluid were removed (Figure 3) to significantly reduced the thrombus burden and restored TIMI 3 flow (Figure 4) reduce ST segment elevation. The vessel was subsequently stented with a 5.0x24mm Liberte bare metal stent (Boston Scientific, USA) at 15atm achieving a good result (Figure 5). There was distal plaque shift which improved somewhat after another run using the Export catheter followed by low pressure dilation with a 5.0x15mm balloon.
Conclusion(s) / Result(s)
The residual clot was not further intervened while iv infusion of glycoprotein IIb/IIIa inhibitor was kept running for the next 18 hours.
Comments/Lessons
N/A
Gallery


Conflicts of Interest
None
Comments