Using One Catheter Treats LAD CTO Through Septal Branch via Transradial Approach, Tip in
by
Leisheng Ru
April 20, 2015Operator(s)
Leisheng Ru, MD, PhD
Affiliation
Cardiovascular Department, Bethune International Peace Hospital, ShijiaZhuang, Hebei, China
Facility / Institute
Cardiovascular Department, Bethune International Peace Hospital,ShijiaZhuang,Hebei,China
Clinical History
A 66-year-old woman presented with chest pain and chest distress for 1 year.She had hypertension and hyperlipipemia as her coronary risk factors.Her baseline ECG showed QS type on V1-V4 leads .Baseline echocardiogram showed LA is 34mm,LV is 52mm; hypokinesia of anterior ventricular wall; LVEF is 47%.
Angiography
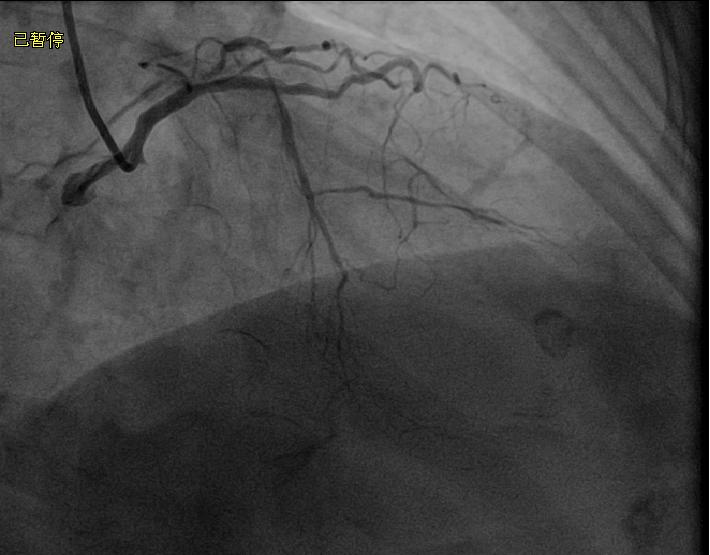
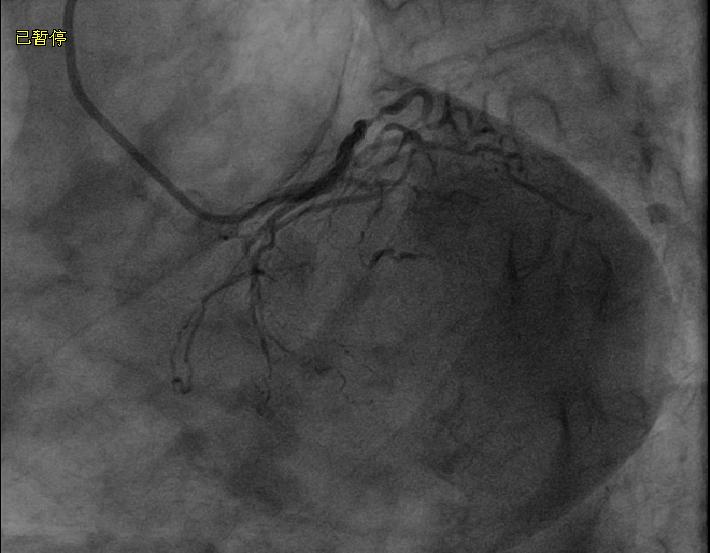
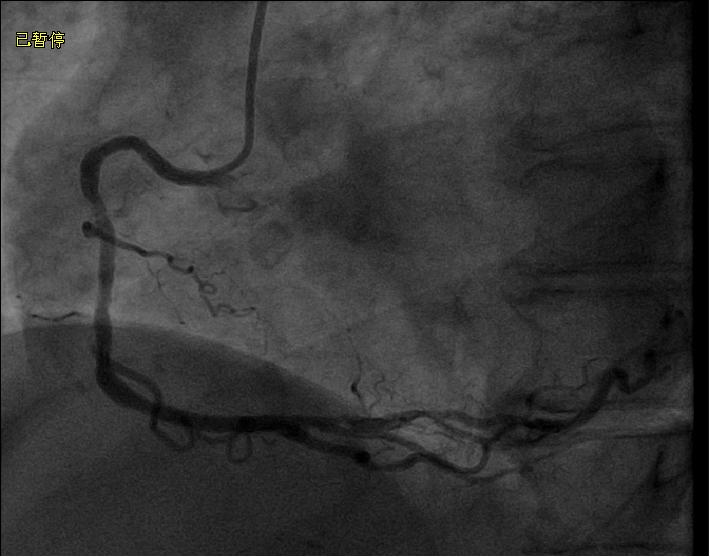
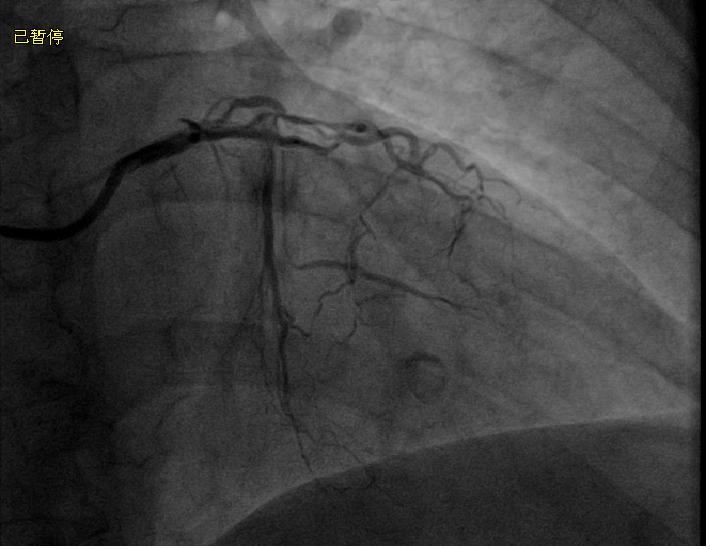
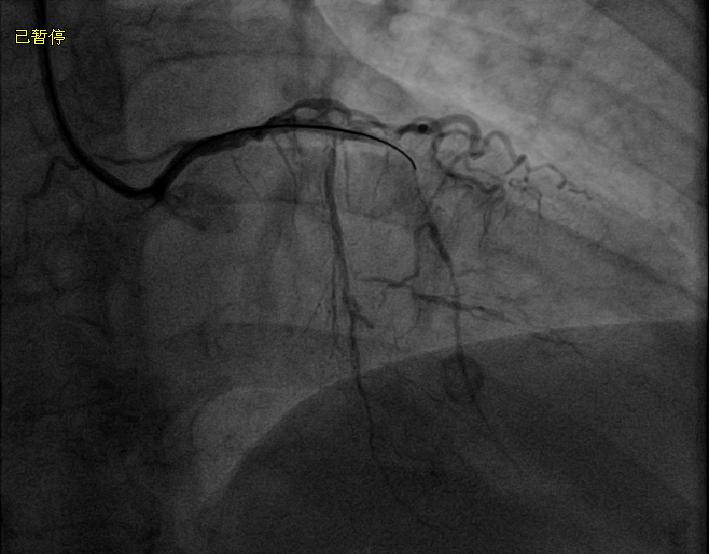
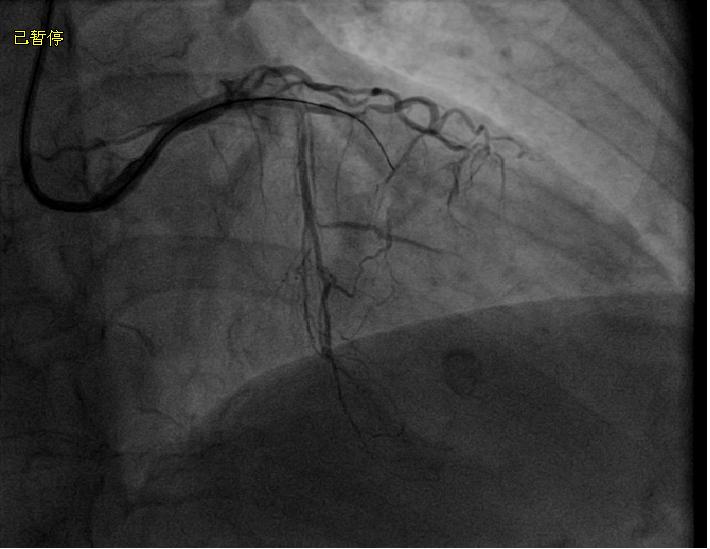
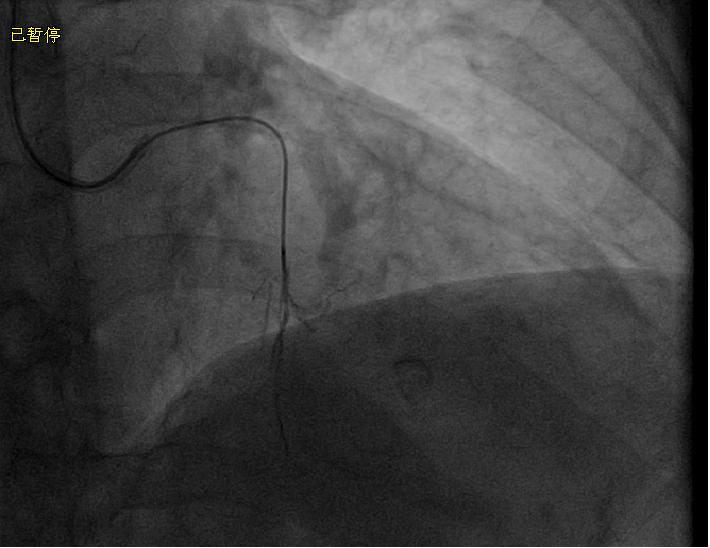
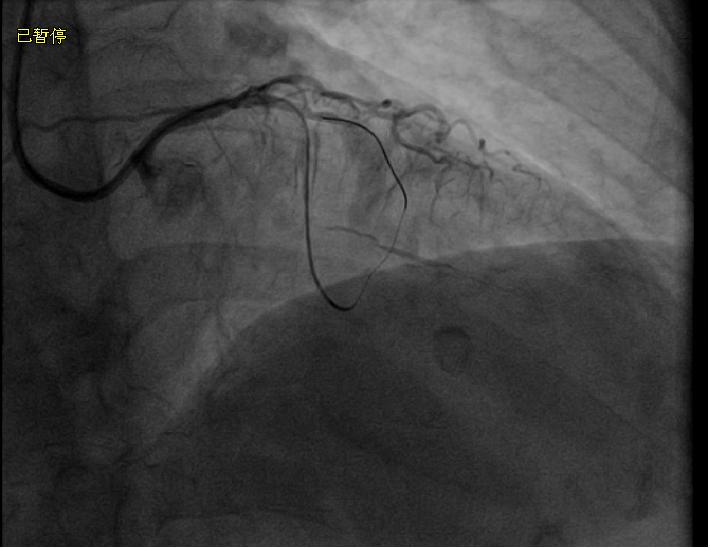
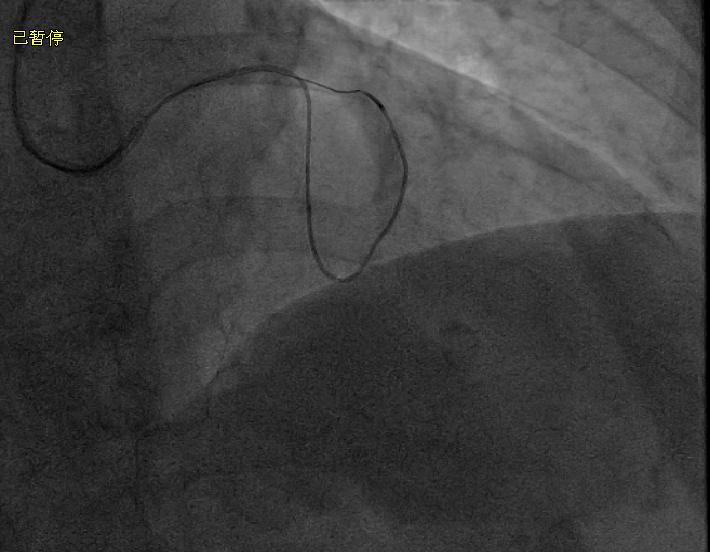
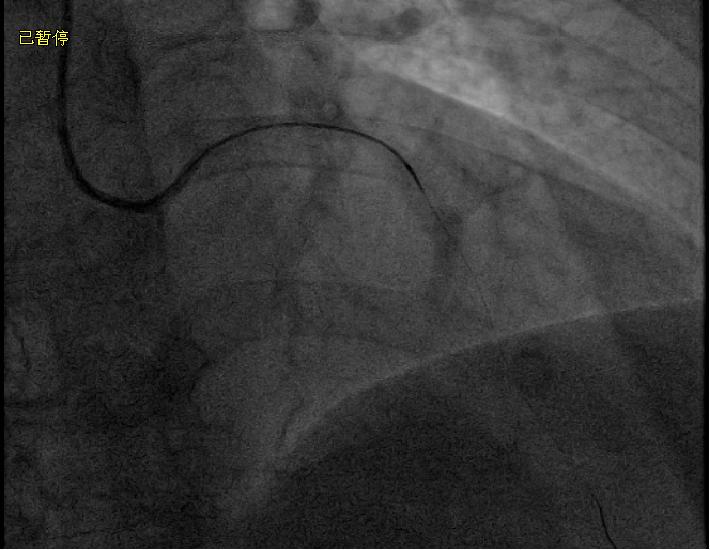
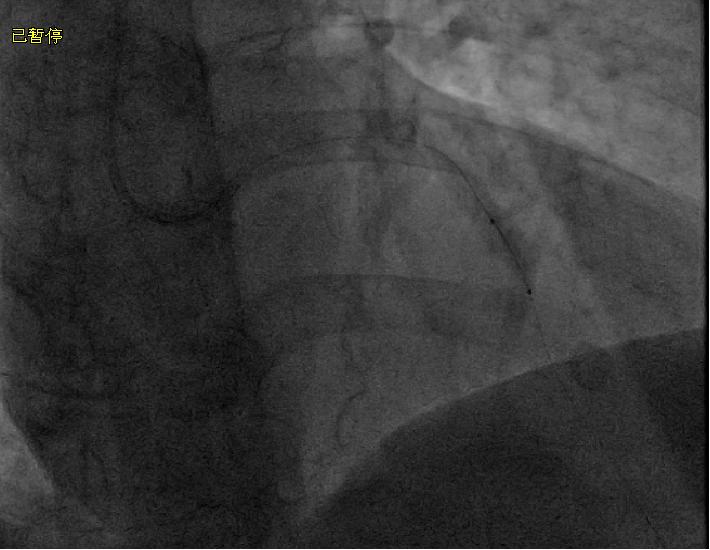
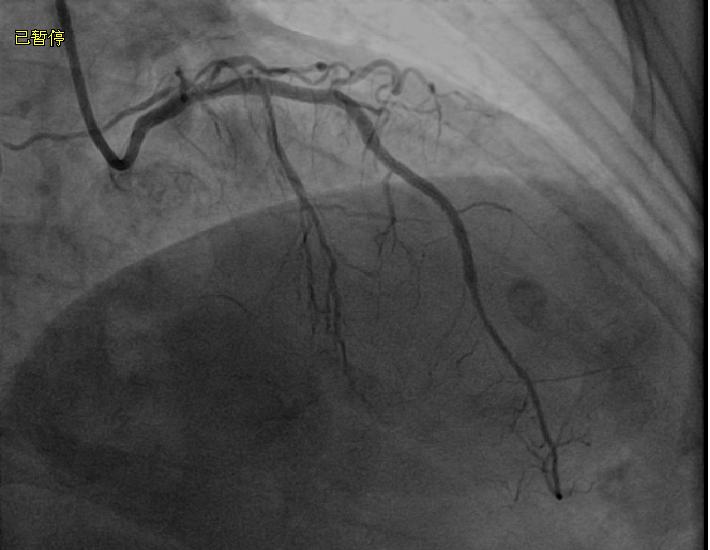
The initial left coronary angiogram showed total occlusion of middle left anterior descending artery (LAD, Figure 1 and Figure 2); and total occlusion of left circumflex (LCX Figure 3).The right coronary angiogram showed a mild to moderate diseased right coronary artery(RCA) (Figure 4).
Procedure
Via the right radial artery, the left coronary was engaged with a 6 Fr JL3.5 guiding catheter.A corsaire was used to increase intralumen support (Figure 5).At first,a 0.014 inch miracle12 guide wire was penetrated into the proximal chronic total occlusion(CTO)segment (Figure 6).Then a Fielder XT and a conquest pro guide wire was respectively replaced to negotiate the lesion but all could't get the LAD true lumen (Figure7 and Figure 8).A retrograde approach was attempted.Firstly,a collateral retrograde angiogram was performed with the corsaire and a big septal branch was seen (Figure 9).The retrograde angiogram showed good collateral flow from the septal branch to middle LAD.A sion guide wire was passed retrogradely to get the proximal true lumen in middle LAD (Figure 10) .Then the corsaire was advanced into the true lumen of proximal LAD. A whisper guide wire penetrated easily into the tip of the corsaire under a vertical projection view ,we call this step the tip-in technique (Figure 11).Then the wire was advanced successfully into the distal septal branch (Figure 12). A 1.5*10mm balloon was inflated to dilate the CTO lesion (Figure 13).From antegrade approach,the corsaire was advanced to the distal true lumen of LAD.The wire was also adjsted to the distal LAD (Figure 14).A 2.0*15mm balloon was dilated (Figure 15) and a 2.5*33mm drug-eluted stent(DES) and a 2.75*33 DES were deployed (Figure 16).Final angiogram showed successful revascularization at LAD CTO segment.
Conclusion(s) / Result(s)
Tip-in technique is very useful in retrograde percutaneous coronary intervention,espetially in transradial approach.Using this technique makes the success rate of CTO via radial approach high.
Comments/Lessons
1.Tip-in technique can avoid the use of retrograde wire externalization,thus save operation time and decrease X volume.
2.The technique decreases the complications of retrograde wire externalization.
The key point:
To tip in corsaire ,we must make the tip of corsaire against the wall of catheter or vessel.
Projection view plays an important role to make sure tip of the corsaire is agaist the catheter or vessel.On the vertical projection view, it takes 1 minute on the average, 5 minutes at the most to finish the tip-in.
2.The technique decreases the complications of retrograde wire externalization.
The key point:
To tip in corsaire ,we must make the tip of corsaire against the wall of catheter or vessel.
Projection view plays an important role to make sure tip of the corsaire is agaist the catheter or vessel.On the vertical projection view, it takes 1 minute on the average, 5 minutes at the most to finish the tip-in.
Gallery



Conflicts of Interest
None
Comments