Cardiac Abnormalities Seen After COVID-19, but Recovery Is Quick
In people who mostly recovered at home, heart inflammation was mild and transient, which experts say is reassuring.


A small proportion of people who recover from COVID-19 have some degree of myocardial inflammation that is linked to abnormalities on cardiac MRI, according to the results of a new study.
Importantly, however, all patients who had evidence of inflammation on 18F-fluorodeoxyglucose positron emission tomography (FDG-PET) showed signs of improvement when reassessed at follow-up.
“We read with great interest the initial studies that came out describing myocardial injury in patients with COVID,” lead investigator Kate Hanneman, MD, MPH (Toronto General Hospital/University Health Network, Canada), told TCTMD. “Even in March 2020, there were early reports about elevated troponin levels in a substantial number of people who were hospitalized with COVID-19. We became interested very early on about whether there was some subclinical damage in the hearts of patients who had more mild disease.”
Senior researcher Paaladinesh Thavendiranathan, MD (Toronto General Hospital/University Health Network), said concerns about the effects of COVID-19 on the heart largely began with ICU patients. In some of the earliest reports from China, for example, data showed that ICU patients had elevations in cardiac troponin and fared worse than those without enzymatic elevations, he told TCTMD.
The major concern is that COVID-19 can lead to long-term changes in the heart, although the extent and significance of subclinical cardiac changes in less-sick patients is still largely unknown.
To date, there have been several cardiac MRI studies in a range of patients with COVID-19, from those hospitalized with the virus to young student athletes who tested positive for SARS-CoV-2. In 2020, one particular study by Valentina Puntmann, MD, PhD (University Hospital Frankfurt, Germany), and colleagues caused a stir when it reported that roughly three-quarters of patients who recently recovered from COVID-19 had evidence of MRI abnormalities and 60% had ongoing myocardial inflammation.
Linking PET Findings to MRI
The range of cardiac MRI abnormalities documented in different studies is likely the result of studying different patient populations, as well as the timing of testing after COVID-19 infection, said Hanneman. FDG-PET, which is more commonly used in oncology and for the assessment of cardiac sarcoidosis, is a sensitive and reliable test to characterize myocardial inflammation, she noted, adding that combined PET/MRI allowed the researchers “to co-register the images so that we can see where the PET abnormality lines up with the MRI abnormality.”
In the new study, published January 12, 2022, in JAMA Cardiology, researchers recruited 47 patients (mean age 43 years; 51% women) who had a positive SARS-CoV-2 test at their hospital to undergo cardiac PET/MRI and blood biomarker assessment within 3 months of the positive test. The majority of patients (85%) recovered at home during the acute infection, nine were admitted to the hospital ward, and three were admitted to the ICU. Prior to PET/MRI, 13 people had received at least one dose of a COVID-19 vaccine (three had two doses).
Right now, there is no evidence to suggest that everyone should be undergoing routine cardiac investigation. Kate Hanneman
In the series, FDG uptake on PET was positive in eight of the study participants. Those with focal FDG uptake had a higher prevalence of hypertension compared with those without evidence of inflammation. Those with FDG uptake also were more likely to have cardiac symptoms than those without, although the difference was not statistically significant. There was no difference in the proportion of PET-positive and PET-negative cases by vaccination status.
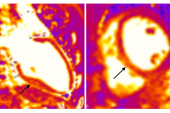
On cardiac MRI, those with focal FDG uptake had a significantly higher prevalence of late gadolinium enhancement (LGE), higher regional T2, T1, and extracellular volume (ECV) plus worse global longitudinal strain and global circumferential strain than those without inflammation. They also had lower LVEFs. Focal FDG uptake colocalized with LGE in four subjects, with high T2 in three patients, with high T1 in three subjects, and with high ECV in two participants. Two people with focal FDG uptake had no evidence of abnormal MRI findings.
High-sensitivity C-reactive protein (hs-CRP), interleukin-6 (IL-6), and interleukin-8 (IL-8), which are markers of systemic inflammation, were higher in patients with focal FDG uptake.
In follow-up imaging on the eight people with PET abnormalities—occurring a mean of 52 days after the initial study—two had a partial resolution of FDG uptake and five had complete resolution (one patient’s test was unreadable due to inadequate diet preparation). All patients had an improvement in LVEF, regional T2, regional T1, ECV, IL-6, IL-8, and hs-CRP.
Long-term Sequelae From Inflammation
To TCTMD, Ron Blankstein, MD (Brigham and Women’s Hospital, Boston, MA), said one of the strengths of the study is that it includes a representative sample of COVID-19 patients who, for the most part, recovered at home. “One of the problems with a lot of studies in imaging is that it’s based on people that are referred,” he said. “A patient with COVID, persistent symptoms, and the doctor refers them for imaging. There’s a huge referral bias.”
With respect to the findings, Blankstein noted that 17% of patients had inflammation documented on PET. While the true prevalence of myocarditis after COVID-19 is debated, and dependent on the patient population, Blankstein said it’s a real condition that does occur in some patients.
“Within this cohort, I would say the incidence of myocarditis is not insignificant,” he said. “At 17%, it’s not large, but it’s still a significant proportion because there’s millions of patients that have been infected with COVID-19. Even if the number was closer to 10%, that would still be a substantial number of individuals who experience myocarditis from COVID.”
The good news, said Blankstein, is that the abnormalities improve, or resolve completely.
“That’s reassuring,” he said. “Most of the abnormalities are mild and transient. As such, we’d expect that the majority of these wouldn’t result in any long-term sequelae for patients. However, that’s obviously one of the areas where we have to study more in the future. It’s always possible, and . . . one of the concerns with myocarditis is that patients have a residual area of scar that could be a focus in the future for arrhythmias.”
Within this cohort, I would say the incidence of myocarditis is not insignificant. Ron Blankstein
Blankstein noted that while inflammatory biomarkers were elevated at the time of imaging in patients with FDG uptake, high-sensitivity troponin I, which was only measured in the hospitalized patients, was not. That finding possibly suggests COVID-19 might have led to inflammation without significant cardiac injury.
Stamatios Lerakis, MD, PhD (Mount Sinai Heart, New York, NY), who also commented on the study for TCTMD, said that a wealth of data over the past 2-plus years have clearly demonstrated that COVID-19 affects the entire cardiovascular system. In this way, the results are not really surprising.
“What is a surprise to me is that myocardial inflammation as detected by PET-FDG was seen 2 to 3 months after the COVID-19 diagnosis,” said Lerakis. “The good news is that this occurred in only a small proportion of participants in the study and appeared to have a good prognosis with resolution at a short-term follow-up.”
Like Blankstein, Lerakis said these findings underscore the need to further study the long-term effects of COVID-19 on the heart. In 2020, Lerakis was part of an international multicenter study that was published in the Journal of the American College of Cardiology showing that myocardial injury was associated with higher in-hospital mortality, particularly if echocardiographic abnormalities were present, although that population included people sick enough to be hospitalized with COVID-19.
Nonspecific Symptoms After COVID-19
The new study has some limitations, including the small sample size and potential for selection bias given that patients volunteered for the study. “It’s possible that patients that had some worry or had some underlying symptoms were more likely to respond compared with the general population of patients with COVID,” said Hanneman.
In terms of public health, she stressed there is no evidence to support widespread cardiac screening in patients who recover from COVID-19, a massive number of people.
“Generally, this should be guided by patients who are symptomatic or who have other signs of cardiac injury,” she said. If an admitted COVID-19 patient had elevated cardiac troponin levels, for example, then further follow-up would be warranted. “Right now, there is no evidence to suggest that everyone should be undergoing routine cardiac investigation,” said Hanneman.
Thavendiranathan agreed.
“As a cardiologist, we have patients referred all the time who have had COVID,” he said, noting that they may be experiencing nonspecific symptoms, such as shortness of breath, chest discomfort, or palpitations. “If you image them, you may find an abnormality which might not even relate to their symptoms or even relate to COVID-19.”
That position against universal screening is endorsed by professional societies, including the Society for Cardiovascular Magnetic Resonance. Right now, the screening strategy for post-COVID-19 patients referred to cardiology is an ECG and echocardiogram to assess for major cardiac abnormalities, said Thavendiranathan.
“One of the hypothesis-generating aspects of our study is the biomarker piece,” he said. “Our patients with a PET abnormality tend to have markers of systemic inflammation.” Although hs-CRP, IL-6, and IL-8 aren’t specific to the heart, if these biomarkers are elevated a month or two after COVID-19, “perhaps these are patients who may benefit from some additional testing, such as MRI or PET,” said Thavendiranathan. “That’s the approach I would take, but of course that would need to be studied.”

Michael O’Riordan is the Managing Editor for TCTMD. He completed his undergraduate degrees at Queen’s University in Kingston, ON, and…
Read Full BioSources
Hanneman K, Houbois C, Schoffel A, et al. Combined cardiac fluorodeoxyglucose-positron emission tomography/magnetic resonance imaging assessment of myocardial injury in patients who recently recovered from COVID-19. JAMA Cardiol. 2022;Epub ahead of print.
Disclosures
- Hanneman reports personal fees from Sanofi Genzyme, Amicus, and Medscape.
- Blankstein reports receiving research funding from Amgen and Novartis; serving on the steering committee for VESALIUS-CV trial (Amgen); and consulting for Caristo Diagnostics Inc.
- Thavendiranathan and Lerakis report no relevant conflicts of interest.
Related News


Comments