Evolut Valves: Initial Positioning Can Be Optimized for Future Coronary Access
It may be possible to deploy the valve in a coronary-access friendly position, experts say.

As transcatheter aortic valve replacement edges toward being a consideration for younger, lower-risk patients, researchers are beginning to think not only about achieving good clinical outcomes during the initial implantation, but also about optimally setting the patient up for future interventions such as PCI.
In a pilot study published July 5, 2019, in Circulation: Cardiovascular Interventions, investigators report on their techniques to reduce the severity of overlap of the transcatheter heart valve commissures with one or both of the coronary orifices, suggesting it may be possible to achieve a more ideal final position of the self-expanding Evolut R and Evolut PRO (Medtronic) devices.
“The issue is that, unlike surgery where we actually remove the leaflets of the aortic valve and put the new valve in and then align the commissures properly, in TAVR nobody has been paying attention to how the valve aligns with the native anatomy,” lead investigator Gilbert Tang, MD (Mount Sinai Health System, New York, NY), told TCTMD. “The focus has been on achieving good outcomes and not whether we need to intervene down the road or to have coronary access in the future. Now, we know that the incidence of coronary artery disease in these younger TAVR patients is quite high. These patients will need to have PCI or at least a diagnostic cath at some point in their lifetime.”
Tang said the prevalence of coronary artery disease in patients with aortic stenosis undergoing TAVR ranges from 40% to 75%, noting that more than 60% of patients in the intermediate-risk trials had coronary disease. The Evolut devices have taller frames than the balloon-expandable Sapien XT and Sapien 3 valves (Edwards Lifesciences), which can make coronary access a potential challenge, he noted.
‘Coronary-Access Friendly’
In their study, the researchers evaluated how the initial deployment orientation of Evolut valves impacted their final position. In doing so, they were able to assess the final orientation of the valve’s commissures in relationship to the coronary arteries. Tang said they also wanted to learn if there was a way to orient the valve at the time of deployment that would translate into a later position that was at least “coronary-access friendly.”
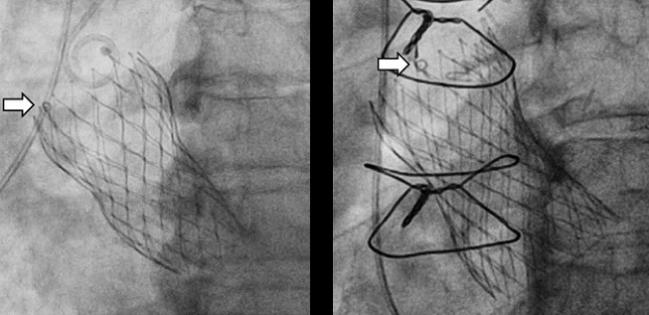
To assess device orientation after TAVR, CT is the gold standard, but rather than exposing patients to additional radiation and contrast, they recorded aortogram images and the final position of the Evolut valve during the procedure. Using the orientation of the C-tab, a marker which represents one of the valve commissures, they co-registered the orientation of the valve to the pre-TAVR CT scan using imaging software so that the orientation of the valve commissures and proximity to the left main and right coronary artery could be determined.
Severe overlap of an Evolut valve commissure with the left main, right coronary, or one or both of these arteries was 33.1%, 20.3%, and 39.0%, respectively. During the initial deployment, when the black capsule “hat” marker on the valve catheter was positioned at the inner curve/center back of the aortic root, severe overlap of the neo-commissures with the left main and right coronary artery was much higher, 63.9% and 52.8%, respectively. In contrast, when the capsule hat marker was positioned on the outer curve/center front of the aortic root, the commissure of the Evolut valves overlapped the left main and right coronary arteries in only 19.5% and 6.1% of cases, respectively.
The problem [for] interventional cardiologists is that we tend to be shortsighted . . . and haven’t really planned out the next 10, 15, or 20 years for some of these younger, lower-risk patients. Christopher Meduri
The implication, according to investigators, is that it may be possible to orient the hat marker to the outer curve/center front position of the aortic root during Evolut R/PRO deployment to reduce coronary overlap. “If the hat marker is located at the inner curve at the time of deployment, or the center-back position, that’s the worst-case scenario,” said Tang. “Almost three-quarters of the time, one of the commissures is placed in front of the coronary arteries. It’s like having a barrier and then you have to go on either side of the commissural post to access the coronary artery. It’s easier said than done.”
The published study includes 118 patients undergoing transfemoral TAVR procedures at two centers and the results have been “pretty consistent” so far, said Tang. And while optimally positioning an Evolut R/PRO device during deployment can facilitate future coronary access, more than 23% of patients had severe overlap of one or more coronary arteries even when optimized with the hat marker in outer curve/center back position during deployment.
Changing Mindset to Focus on the Future
“A lot of interventional cardiologists in the US do not perform TAVR,” said Tang. “There are a lot more PCI centers out there, so it’s important for people to know about this. In emergency situations, with a potential heart attack but there is a previous TAVR, people need to know the orientation of the valve at the time of deployment so that they can find ways to get back into the coronaries more easily rather than struggle with different catheters.”
Christopher Meduri, MD (Piedmont Heart Institute, Atlanta, GA), who was not involved in the study, told TCTMD that TAVR has been established as an excellent therapy for patients at all levels of surgical risk, but that as physicians treat younger patients at lower risk for mortality during surgery, the goal will be to prepare for future procedures.
“One of the issues is coronary reaccess,” he said. “Given that there are only three commercially available valves in the United States and none of them do the alignment automatically like some of the future-generation technologies, trying to do something to optimize [future coronary reaccess] is a novel and important concept. Obviously, it’s far from perfect in accomplishing that, but this is the first step towards at least considering this more and more and hopefully driving industry partners to develop devices that will make it easier.”
The newer-generation devices, such as JenaValve (JenaValve Technology) and J-Valve (JC Medical), are designed to align closer with the native valve commissures but are not currently available in the United States. To TCTMD, Meduri noted that the need for future PCI or a diagnostic catheterization wasn’t even on the radar of investigators in the earliest studies of high-risk and inoperable patients.
“The problem [for] interventional cardiologists is that we tend to be shortsighted and think in terms of immediate results and immediate gratification and [we] haven’t really planned out the next 10, 15, or 20 years for some of these younger, lower-risk patients,” he said. “I think that’s natural since we haven’t been treating people who are going to live 20 or 30 years up until 4 or 5 years ago. It’s a natural progression that as we’re seeing newer issues, we need to start evolving towards them.”
Photo Credit: Adapted from Tang G. Impact of initial Evolut TAVR deployment orientation on final valve orientation and coronary reaccess: a pilot study. Presented at: TVT 2019. June 13, 2019. Chicago, IL.

Michael O’Riordan is the Managing Editor for TCTMD. He completed his undergraduate degrees at Queen’s University in Kingston, ON, and…
Read Full BioSources
Tang GHL, Zaid S, Gupta E, et al. Impact of initial Evolut transcatheter aortic valve replacement deployment orientation on final valve orientation and coronary reaccess. Circulation: Cardiovasc Interv. 2019;Epub ahead of print.
Disclosures
- Tang reports serving as a physician proctor for Edwards Lifesciences and Medtronic.
- Meduri reports serving as a physician proctor for Boston Scientific and Medtronic and serving as a national principal investigator for the Boston Scientific-sponsored REPRISE IV study.
Comments