Four-Dimensional Flow CMR Shows Promise in Aortic Stenosis
This can be an important add-on to echocardiography in patients with a borderline need for intervention, researchers say.

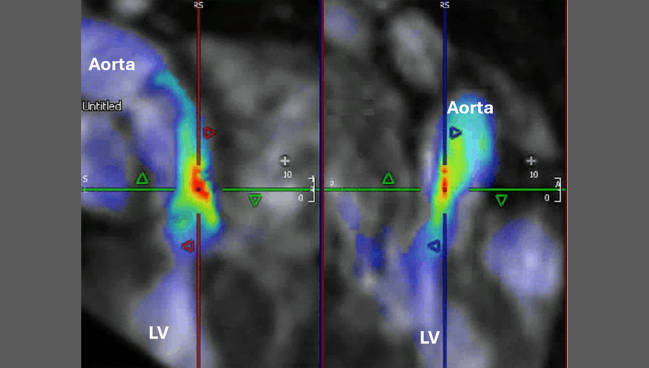
Photo Credit: Pankaj Garg
Four-dimensional flow cardiovascular MRI (4D flow CMR) can more accurately estimate peak aortic valve velocities (VPeak) than traditional transthoracic echocardiography (TTE) in patients with aortic stenosis (AS), according to data from the PREFER-CMR registry.
The findings are encouraging in the context of the recent approval of TAVI for patients with asymptomatic severe AS in the United States, researchers say, because 4D flow CMR could allow for better assessment of pressure drops and flow dynamics across the valve that would, in theory, lead to better clinical outcomes, especially among those with moderate-to-severe disease.
“4D flow allows us to have a bit better precision when you’re thinking about timing of aortic valve intervention,” senior author Pankaj Garg, MD, PhD (Norfolk and Norwich University Hospitals NHS Foundation Trust, Norwich, England), told TCTMD.
“Importantly, what we also realize is . . . when you can’t align the ultrasound to the flow direction, the ultrasound can underestimate the peak velocity, whereas in 4D flow MRI, you’re acquiring that data across the whole cross section,” he explained. “So you have per-pixel information, irrespective of which position they’re lying in and . . . you get that information anyway without any operator dependence.”
Still largely investigational, 4D flow CMR has emerged as a possible addition to the AS imaging tool kit, and the new data add to the evidence base showing that it works, Tom Wang, MBChB, MD (Cleveland Clinic, OH), told TCTMD. “The hope is that there’s more studies on this in the future to try and make use of it more, and then maybe it’ll be more accurate than echo and then we can use it more widely,” said Wang, who was not involved in the new research.
Real-world Patients
For the study, published online last week in Open Heart, lead author Ciaran Grafton-Clarke, MBChB (Norfolk and Norwich University Hospitals NHS Foundation Trust), Garg, and colleagues looked at 30 patients with aortic stenosis who underwent both TTE and 4D flow CMR in the PREFER-CMR registry between February 2021 and January 2022.
Seventeen of those patients underwent an intervention. Those who did tended to be younger than those managed conservatively (mean 72.1 vs 79.9 years), and they had higher left ventricular ejection fraction (P = 0.02) and right ventricular ejection fraction (P = 0.004) on CMR as well as higher mean velocity on TTE (P = 0008).
VPeak was higher for patients who underwent an intervention than for those who did not, both when measured by continuous wave Doppler (CWD; 3.4 vs 2.6 m/s, P = 0.0025) and 4D flow (4.2 vs 2.7 m/s, P < 0.0001). However, only 4D flow VPeak was able to significantly predict whether a patient needed an intervention (HR 2.51; P < 0.01).
Further, the researchers note a moderate positive correlation between CWD VPeak and 4D flow CMR VPeak (R 0.55; 95% CI 0.24-0.76; P = 0.002), with a mean bias of -0.5 m/s (95% CI -0.79 to -0.12; P = 0.01) indicating that CWD “slightly underestimated” the VPeak.
‘It’s Happening’
While the technology to execute 4D flow CMR is currently available for most clinical magnets in use around the US today, the software to analyze the data had “lagged” up until the last few years, Garg said, adding that he is now leading clinical trials that are using 4D flow results as primary endpoints. “It’s happening,” he said, acknowledging that the price and learning curve for 4D flow CMR are steeper than for echocardiography.
The idea is not to use CMR instead of echocardiography, Garg specified. “I think cardiac MR can allow precision where it’s necessary so you can subselect patients, and equally in patients where more precise monitoring is necessary over time because you’re removing the operator dependence here in this technology completely.”
4D flow allows us to have a bit better precision when you’re thinking about timing of aortic valve intervention. Pankaj Garg
Wang agreed, noting that 4D flow CMR will be most useful in patients with moderate-to-severe AS on echocardiography as a way to help determine if an intervention is warranted. “When patients have severe aortic stenosis, as per current guidelines, if they have symptoms, we definitely refer them for surgery or [transcatheter] intervention of some sort,” he said. “But if you’re sort of on the borderline between moderate to severe and your symptoms are uncertain, that’s when we do further tests. . . . This is where the MRI can maybe be another test in the armamentarium to assist.”
It’s hoped that using this imaging technology would lead to cost savings down the line by preventing clinical events that might arise from poor procedural planning or execution, but those studies remain to be completed, Garg added.
He would like to see “more and more sites use [4D flow CMR] and report what they have learned,” as well as industry-sponsored training programs. “What’s hard to appreciate is what can go wrong with this technology,” he continued. “You’re embracing more images, you’re embracing a technology which is much more complex . . . and there are always some trade-offs.”
Wang agreed that there will need to be refinement in processing all the information that CMR can provide and only using what is relevant to managing patients and improving their outcomes. 4D flow CMR also has potential outside the field of valvular heart disease, he added, including implications for cardiomyopathies, congenital heart disease, and CAD.
“This is a very exciting time for cardiac imaging and in multimodality, whether it’s echo, CT, or MRI, with the interface of new technologies trying to make the scan more precise, so better spatial resolution [and] shortening the scan time,” Wang said. “This is a very small study with lots of limitations, but with more experience in larger groups of patients and multicenter collaborations, hopefully that will bring this about to try and improve patient care and their outcomes.”

Yael L. Maxwell is Senior Medical Journalist for TCTMD and Section Editor of TCTMD's Fellows Forum. She served as the inaugural…
Read Full BioSources
Grafton-Clarke, C, Assadi H, Li R, et al. Four-dimensional flow provides incremental diagnostic value over echocardiography in aortic stenosis. Open Heart. 2025;12:e003081.
Disclosures
- Garg reports receiving funding from the Wellcome Trust Clinical Research Career Development Fellowship and serving as a clinical advisor for Pie Medical Imaging and Medis Medical Imaging.
- Grafton-Clarke and Wang report no relevant conflicts of interest.
Related News


Comments