Mortality High in Patients With STEMI, COVID-19 on Hemodynamic Support
North American registry data show a 60% death rate with MCS, which researchers say should enter into informed consent.


Three in five COVID-19 patients with STEMI who require mechanical circulatory support (MCS) will die in the hospital, according to observational data spanning 16 months of the pandemic.
The results, from the North American COVID-19 Myocardial Infarction (NACMI) registry, were presented as a moderated poster during last week’s TCT 2021 meeting in Orlando, FL.
Knowledge of the 60% mortality rate observed with MCS in STEMI can guide informed consent and decision-making, lead author Raviteja Guddeti, MD (Minneapolis Heart Institute Foundation, MN), told TCTMD. In discussions with patients and medical teams, this information can enable participants to say, “If everybody’s on the same page, we can go ahead and use [MCS],” he explained.
What’s still unknown is how high mortality might rise for COVID-positive STEMI with cardiogenic shock were MCS not used, he pointed out.
Earlier NACMI registry data showed a strikingly high death rate—around 33%—for patients diagnosed with COVID-19 on top of having STEMI. There also was the good news that, despite the pandemic’s challenges, most patients have continued to undergo prompt PCI. Yet global registry data have indicated cardiogenic shock was linked to longer ischemic time among ACS patients with COVID-19, and was seen in 75% of those experiencing cardiovascular death.
Guddeti said that, thanks to acute respiratory distress syndrome (ARDS) being a common manifestation of COVID-19, more data have been gathered about venovenous extracorporeal membrane oxygenation (ECMO). Far less is understood about how venoarterial ECMO and other forms of hemodynamic support are being used in COVID-19 patients who’ve experienced STEMI complicated by cardiogenic shock.
MCS Used in 13%
This analysis looked at 1,043 STEMI patients enrolled in NACMI from January 2020 to April 2021. Among them, 36% were diagnosed as COVID-positive, while the rest, the non-COVID group, tested negative after being suspected of having the disease.
MCS was used in 13.3%, with no difference between the COVID and non-COVID populations.
Most COVID-19 patients were from ethnic minority groups (54%). Yet those receiving MCS tended to be Caucasian (63%). “That’s actually a pretty remarkable difference, Guddeti said. “We’re trying to look at that further. . . . Is it something to do with their presentation, how sick they are? Something to do with their insurance coverage? Something to do with where they present? We don’t know that yet.”
Additionally, Guddeti drew attention to the shock severity. All of the MCS-treated patients were in Society for Cardiovascular Angiography and Interventions class D or E, indicating a deteriorating or extremis condition. “None of them were even class C,” he observed.
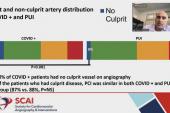
Most baseline and treatment characteristics were similar irrespective of COVID-19 status, though dyslipidemia was less prevalent in the COVID-positive patients (34% vs 61%; P = 0.003), as was cardiac arrest before PCI (18% vs 36%; P = 0.033). The COVID-19 patients also were more likely to not undergo angiography (6% vs 0%; P= 0.042) and less likely to undergo CABG (5% vs 13%; P = 0.013).
In those receiving MCS, intra-aortic balloon pump (IABP) was the most common type. Within the COVID-19 group, MCS type was 53% IABP, 24% ECMO, 16% Impella (Abiomed), and 8% a combination. ECMO was less frequently used in the non-COVID group, making up just 3% of MCS.
The primary outcome—a composite of in-hospital mortality, stroke, recurrent MI, or unplanned revascularization—occurred at a higher rate in those with versus without COVID-19, driven by a difference in all-cause death.
In-Hospital Outcomes of MCS Patients
|
|
COVID-19 |
No COVID-19 |
P Value |
|
Primary Endpoint |
60% |
30% |
0.001 |
|
All-Cause Death |
59% |
28% |
0.001 |
|
Reinfarction |
3% |
3% |
1.00 |
|
Repeat Angiogram |
16% |
12% |
0.575 |
|
Stroke |
5% |
4% |
0.662 |
Beyond informed consent, their data could factor into debates over whether “to initiate MCS in the face of limited resources during the pandemic,” the poster notes.
The answer to the question of how to weigh the mortality risk may depend on where patients initially present, said Guddeti. At tertiary and quaternary centers with more resources, “they’ll be able to afford placing the devices and seeing how things work out,” he suggested, as “compared with a mid-level center where they may hesitate a little more.”

Caitlin E. Cox is Executive Editor of TCTMD and Associate Director, Editorial Content at the Cardiovascular Research Foundation. She produces the…
Read Full BioSources
Guddeti R. Mechanical circulatory support in COVID-19 patients presenting with myocardial infarction: analysis from the North American COVID-19 Myocardial Infarction registry. Presented at: TCT 2021. Orlando, FL. November 4, 2021.
Disclosures
- Guddeti reports no relevant conflicts of interest.
Related News


Comments