Outcomes Worse With Combined Transcatheter Aortic, Mitral Procedures
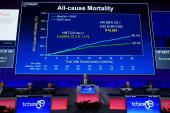
In-hospital mortality was higher when TEER or TMVR were done during the same hospital stay as TAVI, compared with TAVI alone.


Patients who undergo a transcatheter mitral valve intervention during a hospital stay that also includes TAVI fare worse over the short term than those who only receive an aortic intervention, an analysis of administrative claims data show.
In-hospital mortality was significantly greater in patients who underwent both TAVI and either transcatheter edge-to-edge repair (TEER) of the mitral valve or transcatheter mitral valve replacement (TMVR), lead author Ayman Elbadawi, MD (University of Texas Medical Branch at Galveston), and colleagues report in a JACC: Cardiovascular Interventions research letter.
Combined procedures—which were rare, accounting for just 0.1% of TAVI admissions during the study period—also were associated with greater use of mechanical circulatory support, higher rates of acute kidney injury, discharge to nursing facilities, and longer hospital stays.
“So it appears based on these data that these combined procedures are being done in the United States, but they’re associated with increased risk of in-hospital mortality and morbidity compared with TAVR alone,” senior author Sachin Goel, MD (Houston Methodist Hospital, TX), told TCTMD.
Part of that might be due to combined procedures being more likely in urgent or emergent situations, Goel said, noting that transcatheter aortic and mitral interventions are typically done electively.
“Urgent or emergent TAVR is feasible in a select group of patients, but both procedures at the same time may be a bit of a stretch,” he said, adding that “there must have been a strong reason why both procedures were done at the same time.”
The usual practice is to perform TAVI first and then see if any potentially treatable mitral regurgitation (MR) resolves, which is thought to occur about half of the time, Goel explained. Patients with persistent severe MR weeks or months after TAVI are then evaluated for a transcatheter mitral procedure.
Goel noted, however, that “surgery is equally important” to consider in patients with severe aortic stenosis (AS) and MR. “If they have severe AS and moderate-or-more mitral regurgitation at baseline, if their surgical risk is not very high, perhaps they should be considered for double valve surgery.”
But the best treatment strategy isn’t clear, he indicated, saying “this patient population deserves further study to evaluate the optimal treatment approach up front.”
National Readmissions Database
Many patients undergoing transcatheter or surgical intervention for severe AS have concomitant MR, Goel noted. The surgical literature indicates that outcomes of operating on both valves “are not that great,” especially in older patients with comorbidities, but less is known about the impact of combining transcatheter interventions.
To explore the issue, the investigators turned to the National Readmissions Database, identifying 210,181 hospitalizations for TAVI between 2014 and 2018. A small percentage of those admissions also involved TEER (0.05%) or TMVR (0.05%).
In most cases, the mitral procedure was done on the same day as TAVI—68% for TEER and 92.8% for TMVR. Generally, patients who underwent combined procedures were younger and more likely to have a variety of comorbidities, including heart failure, compared with those treated with TAVI alone. Nonelective admissions were more common with combined procedures, a difference that was significant in the TEER group (54.6% vs 19.7%; P = 0.01), but not in those who underwent TMVR (30.2% vs 19.7%; P = 0.09).
Moreover, combined TAVI/TEER was associated with higher rates of cardiac arrest, use of mechanical circulatory support (MCS), acute kidney injury, new hemodialysis, major bleeding, blood transfusion, and discharge to nursing facilities (adjusted ORs ranging from 2.26 to 5.65). Similarly, combined TAVI/TMVR was associated with higher rates of MCS use, acute kidney injury, and discharge to nursing facilities (adjusted ORs ranging from 2.05 to 4.61). Median length of stay also was longer with combined procedures (median 8 vs 3 days; P < 0.001).
Keeping the Data in Mind
The researchers note that there is some evidence that performing staged TEER or TMVR in patients with significant residual MR after TAVI is feasible and safe, citing a multicenter registry study and a systematic review. The current study demonstrating an increase in in-hospital mortality with combined procedures differs in that it assesses outcomes when the aortic and mitral interventions are done during the same hospitalization.
“The higher risk of in-hospital mortality associated with combined transcatheter interventions for aortic stenosis and MR is likely multifactorial and related to cumulative risk of the two procedures in the elderly and often frail patients, increased burden of comorbidities, and higher frequency of nonelective admissions (in the TEER group) indicative of a sicker patient population compared with those undergoing elective TAVR alone,” Elbadawi et al write.
Goel said “these are important data to keep in mind” when navigating this clinical scenario. “While in some of these patients we can logistically do both procedures, these are sick patients, and [the combination of procedures is] associated with high mortality.”
He acknowledged that the study was limited by the use of an administrative database that lacks information on postdischarge outcomes and imaging, as well as procedural details.

Todd Neale is the Associate News Editor for TCTMD and a Senior Medical Journalist. He got his start in journalism at …
Read Full BioSources
Elbadawi A, Elgendy IY, Afify H, et al. Combined transcatheter aortic and mitral valve interventions: insights from a national database. J Am Coll Cardiol Intv. 2021;14:1500-1507.
Disclosures
- Goel reports being on the speakers bureau for Abbott Structural Heart and being a consultant for Medtronic.
- Elbadawi reports no relevant conflicts of interest.
Related News


Comments