PREPARE-CALC Shows Benefits of Rotational Atherectomy
Newer-generation DES might be at the root of the positive results, researcher says.
SAN DIEGO, CA—Lesion preparation with upfront high-speed rotational atherectomy is safe, feasible, and more often successful as a primary strategy before DES implantation compared with modified balloon angioplasty in patients with severely calcified lesions, according to the PREPARE-CALC study.
“In patients with severely calcified coronary lesions, upfront elective rotational atherectomy is feasible in nearly all patients and the acute success rate is superior to modified balloons, but both elective rotational atherectomy and modified balloons with potential bailout rotational atherectomy are equally safe and effective. And, use of rotational atherectomy is no longer associated with excessive late lumen loss in the era of modern sirolimus-eluting stents,” Gert Richardt, MD (Heart Center, Segeberger Kliniken, Bad Segeberg, Germany), who presented the results during a Late-Breaking Clinical Science session last week at TCT 2018.
Of 200 patients enrolled in the randomized controlled trial, 100 were assigned lesion preparation with modified balloon angioplasty or with rotational atherectomy. The primary endpoint of strategy success, which was powered for superiority, occurred more often with atherectomy than with modified balloons (98% vs 81%; P = .0001). The main driver of strategy failure in the modified-balloon group was the need to cross over to rotational atherectomy (16% vs 0%; P < 0.0001). The most common causes for crossover were uncrossable or undilatable lesions.
In prespecified subgroup analysis, the researchers identified three groups with a significant interaction with the intervention that resulted in no advantage of rotational atherectomy: women (P = 0.03), patients with left anterior descending coronary artery as the target vessel (P = 0 .002), and those with non-type C lesions (P = 0.001).
Unlike in previous studies, rotational atherectomy was not associated with excessive late lumen loss in PREPARE-CALC, Richardt said. At 9 months, the co-primary endpoint of mean in-stent late lumen loss was not significantly different between the rotational-atherectomy and modified-balloon groups (P = 0.21; P for noninferiority = 0.01).
Clinical outcomes at 9 months also did not differ significantly, with Richardt emphasizing the low rate of target vessel failure in both treatment groups.
The PREPARE-CALC study enrolled patients with severely calcified CAD amenable to PCI from 2014 to 2017. Baseline characteristics were fairly balanced between groups, with the exception of more left main disease in the modified-balloon group (P = 0.03). Angiographic and procedural characteristics were also mostly similar between groups; however, the use of 7-Fr guiding catheter and balloon predilatation were more common in the rotational atherectomy group, and maximum stent implantation pressure was higher in the modified balloon group.
In the modified-balloon group, the most frequently used device was the AngioSculpt Scoring Balloon (AngioScore), followed by the Scoreflex Scoring Balloon (OrbusNeich Medical) and the Flextome Cutting Balloon (Boston Scientific). Rotational atherectomy was performed using Rotablator (Boston Scientific). Burr size was selected to reach a burr-to-vessel ratio of 0.5, and rotational speed ranged from 140,000 to 180,000 rotations per minute. New-generation sirolimus-eluting stents with a bioabsorbable polymer (Orsiro; Biotronik) were used for DES implantation.
New Techniques, New Technologies?
The study had several limitations, Richardt noted, including crossover as a potential source of bias, predominant use of the transfemoral approach, exclusion of acute and clinically unstable patients, and angiography-guided procedures. Additionally, it was not powered for clinical endpoints and did not evaluate newer techniques, such as orbital atherectomy and laser lithoplasty.
During a roundtable discussion following the presentation, one panelist said the lack of late lumen loss was “really surprising” and questioned whether new techniques may be responsible for this finding. Richardt pointed out, however, that the techniques used in PREPARE-CALC were not significantly different from those used in the 2012 ROTAXUS trial and therefore postulated that the difference lies in the newer-generation DES used.
Another panelist also questioned whether the new technologies that were not studied could be even safer.
“I was a believer in these new technologies, but when I saw very low event rates after 9 months in this study, I asked myself: What is the additional effect that we can create with these new technologies? Is there still an unmet need that we have to address with these new technologies or are our old tools, if used in the right way, able to achieve good results?” Richardt said.
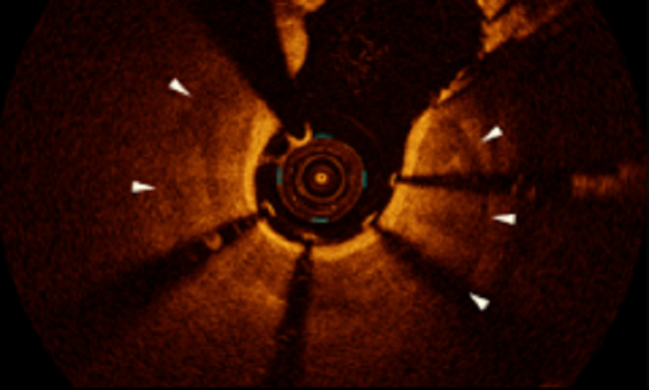
Photo Credit: Richardt G. PREPARE-CALC: a randomized trial of high-speed rotational atherectomy prior to drug-eluting stent implantation in severely calcified coronary lesions. Presented at: TCT 2018. September 24, 2018. San Diego, CA.
Sources
Richardt G. PREPARE-CALC: a randomized trial of high-speed rotational atherectomy prior to drug-eluting stent implantation in severely calcified coronary lesions. Presented at: TCT 2018. September 24, 2018. San Diego, CA.
Disclosures
- Richardt reports speaker’ honoraria from Boston Scientific and Biotronik.
Comments