Simple, Phone-Based Strategy Improves BP Control in Stroke Survivors
The intervention, tested out in Ghana, is unique as it relies on basic mobile phones, not smartphones.

HELSINKI, Finland—In Ghana, survivors of a recent stroke who had hypertension experienced significant improvements in blood pressure control with a simple, mobile-health (mHealth) intervention led by nurses, according to the results of the PINGS-2 trial.
After 1 year, 67% of patients managed with the intervention had a systolic BP below 140 mm Hg, compared with just 43% of those managed with usual care (P < 0.001), Bruce Ovbiagele, MD (University of California, San Francisco), reported last week at the European Stroke Organisation Conference (ESOC) 2025
The strategy involved use of basic mobile phones, in contrast to several prior studies conducted in the United States and the United Kingdom that used smartphones with Bluetooth technology, he noted.
“This is a relatively simple, rudimentary approach that we’ve taken, but [it] is contextually appropriate,” Ovbiagele said during his presentation. “To our knowledge, this is the first large multicenter study of this kind that has been done in the region.”
He added that because there is a national healthcare system in Ghana, which is not typical in Africa, the nurse-led mHealth intervention used in PINGS-2 potentially “could be scalable” for recent stroke survivors throughout the country. “But we also think in pockets in Africa, there might be an opportunity where some aspects of the intervention might be transferable or adaptable for use in those settings as well,” said Ovbiagele.
The PINGS-2 Trial
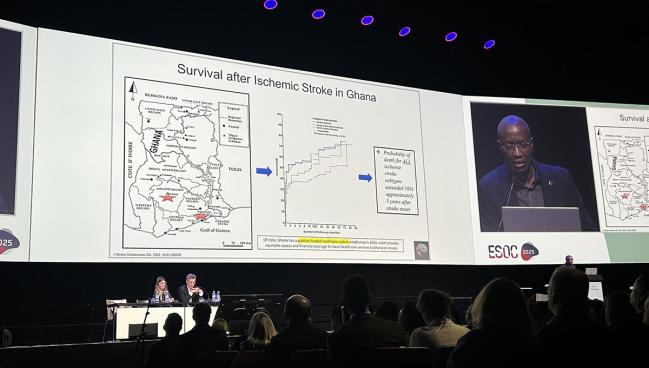
Stroke have been rising across Africa, and in Ghana specifically, rates of ischemic and hemorrhagic stroke have increased by about 18% and 20%, respectively, over the past two decades, Ovbiagele said. Mortality after stroke also is high, he added.
In Ghana and other parts of Africa, the control of BP after stroke is “extremely poor” due to several factors, including fragmentation of the healthcare system, overburdened workers, a paucity of physicians, and a lack of affordable drugs, Ovbiagele said. Issues at the patient level, including a lack of knowledge about how to take medications or how not to use them in conjunction with traditional remedies, are at play as well.
There is good penetration of mobile phones across Africa, and prior studies have examined whether mHealth interventions can improve outcomes on the continent. These have mostly focused on cancer and diabetes, and the few hypertension studies that have been done have been single-center pilot studies of short duration, according to Ovbiagele.
An initial PINGS pilot trial performed by Ovbiagele’s group in Ghana demonstrated the feasibility of deploying a nurse-guided, mobile phone-based intervention among stroke survivors and hinted at an improvement in BP control. However, the study used smartphones, which had to be loaned to about half of the participants.
The phase III PINGS-2 trial instead used basic mobile phones for the intervention. For the study, which was conducted at 10 hospitals in Ghana, Ovbiagele and colleagues enrolled 500 patients (mean age 59 years; 43% women) who were less than a month out from an ischemic or hemorrhagic stroke, had uncontrolled BP (140/90 mm Hg or higher), and owned a mobile phone that could receive texts and audio messages.
About three-quarters of participants had had an ischemic stroke. At baseline, the median NIHSS score was 3 and the median modified Rankin Scale score was 2. Mean BP was roughly 158/95 mm Hg.
The PINGS intervention included three main parts. Patients were given home BP monitors and taught how to use them, with nurses performing weekly case management assessments. Phone alarms were set as medication reminders. In addition, patients and/or caregivers received weekly audio messages that included education about cardiovascular risk reduction. Patients in the usual-care control group also received the weekly audio messages, but not the other components of the intervention.
The primary outcome was the proportion of patients with a systolic BP below 140 mm Hg by 1 year: patients in the control group were significantly less likely to meet this goal (RR 0.64; 95% CI 0.54-0.75). The finding was consistent across subgroups defined by sex, education, income, diabetes, body weight status, age, stroke type, health facility, renal function, and baseline systolic BP.
Patients in the intervention group had a significantly lower mean systolic BP at 1 year (138 vs 143 mm Hg; P = 0.008) and a greater mean decrease over that span (20 vs 14 mm Hg; P = 0.016). There was no difference in diastolic BP. That is “a little bit surprising,” Ovbiagele said, although he noted that 28% of the cohort had isolated systolic hypertension and the aim of the protocol was to reduce systolic BP.
The rate of major adverse cardiovascular events, including recurrent strokes, coronary artery disease, and vascular deaths, was not significantly different between the intervention and control groups (6.6% vs 4.7%; P = 0.50).
Ovbiagele noted that longer-term follow-up, which is ongoing in the trial, is important to test the durability of the intervention because people can get tired of receiving text messages. In addition, his group plans to examine implementation outcomes to assess what worked with the intervention.
“And then finally, we would like to move to the next step. As you might have seen, 67% had control at 1 year, which is not great, but is great for the region,” Ovbiagele said. “We’d like to develop more effective interventions and also target a systolic blood pressure of less than 130, which is much more consistent with the guidelines.”

Todd Neale is the Associate News Editor for TCTMD and a Senior Medical Journalist. He got his start in journalism at …
Read Full BioSources
Ovbiagele B. Efficacy of blood pressure control among stroke survivors over 12 months via a nurse-navigator, mHealth-enabled intervention in Ghana: a phase III multicenter clinical trial. Presented at: ESOC 2025. May 22, 2025. Helsinki, Finland.
Disclosures
- The trial was funded by the US National Institutes of Health/National Heart, Lung, and Blood Institute.
- Ovbiagele reports no relevant conflicts of interest.
Related News



Comments