STEP Trial Supports Lower BP Goal in Older Patients With Hypertension
The findings confirm those from SPRINT but don’t address what to do in very elderly patients, one expert says.

Intensive lowering of blood pressure (BP) reduced cardiovascular events in an older Han Chinese population in the STEP trial, providing confirmation of the benefits seen earlier in the SPRINT trial, experts say.
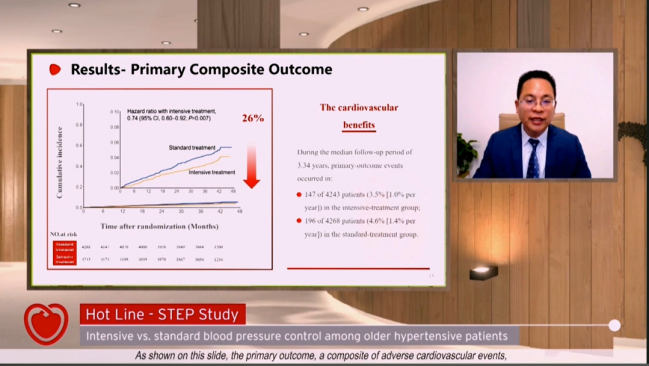
Aiming for a systolic BP goal of 110 to less than 130 mm Hg versus a goal of 130 to less than 150 mm Hg led to a 1.1% absolute reduction in risk of a composite of stroke, ACS, acute decompensated heart failure, coronary revascularization, atrial fibrillation (AF), or CV death (3.5% vs 4.6%; HR 0.74; 95% CI 0.60-0.92). Jun Cai, MD, PhD (Fuwai Hospital, Beijing, China), reported the results during the virtual European Society of Cardiology Congress 2021.
Most of the individual components of that primary endpoint favored intensive treatment, although there were no significant between-group differences in coronary revascularization, AF, or CV death. All-cause death occurred at similar rates in the intensive and standard arms (1.6% vs 1.5%).
More-aggressive control of BP was well tolerated in the trial, with no differences in most adverse events (including dizziness, syncope, and fracture, angioedema, headache, cough, and hives) or adverse renal outcomes; hypotension was increased in the intensive group (3.4% vs 2.6%; P = 0.03).
The findings, published simultaneously online in the New England Journal of Medicine, “support that for older patients, the [systolic BP] target should be set lower than 130 mm Hg for better cardiovascular benefits,” Cai said at a media briefing.
For Donald Lloyd-Jones, MD (Northwestern University Feinberg School of Medicine, Chicago, IL), president of the American Heart Association (AHA), “this trial is an important confirmation of the approach taken in the SPRINT trial to show us that achieving a systolic blood pressure less than 130 is associated with substantially lower risks than achieving the old target of less than 140.”
A systolic goal below 130 mm Hg has a class I recommendation in the hypertension guidelines from the AHA, the American College of Cardiology, and nine partnering organizations, with a level of evidence B-R, indicating moderate-quality evidence from one or more RCTs. Lloyd-Jones suggested to TCTMD that the STEP trial could result in the strengthening of that recommendation to include level of evidence A.
“And what we know about recommendations that get level of evidence A is it is very rare that they get overturned, because it would take a huge trial with a very different unexpected result to overturn the weight of evidence that’s now gathered here,” he said. “So I think going forward we’re going to see more and more recommendations to shoot for a target of less than 130, and we’re going to be increasingly confident that that’s the right thing to be doing, because we’ve got now at least these two large trials that have specifically targeted that less-than-130 area.”
There remains some debate in the hypertension community about the appropriate treatment goal for older patients, however. Chinese guidelines, as well as those from the American College of Physicians/American Academy of Family Physicians, call for a systolic goal of less than 150 mm Hg for older adults, whereas European guidance states that the initial objective is to bring BP below 140/90 mm Hg in all patients, with a goal of 130 to 140 mm Hg in patients older than 65 if treatment is well tolerated.
The STEP Trial
In the STEP trial, the investigators set out to provide some clarity. At 42 centers in China, they enrolled 8,511 hypertensive patients ages 60 to 80 (mean age 66.2 years; 46.5% men) and randomized them to the intensive or standard systolic BP goal. BP was measured both in the office by trained clinicians using validated Omron electronic sphygmomanometers and at home using a monitor paired with a smartphone app. Overall, 19.1% of patients had a history of diabetes, 6.3% had a history of CVD, and 64.8% had a Framingham risk score of 15% or higher. Average BP at baseline was about 146/83 mm Hg.
So I think this tells us that in the majority of patients, we should be shooting for these lower blood pressure targets, as suggested in the American guidelines. Donald Lloyd-Jones
During a median follow-up of 3.34 years, intensive treatment resulted in a systolic BP that was an average of 9.2 mm Hg lower than in the standard arm (126.7 vs 135.9 mm Hg). By 3 years, 77.2% of patients getting more-aggressive treatment achieved a goal between 110 and 130 mm Hg.
That BP difference translated into a significant reduction in the primary composite outcome, and half of the individual components, in the intensive-treatment arm.
Outcomes Based on BP-Lowering Strategy
|
|
Intensive (n = 4,243) |
Standard (n = 4,268) |
HR (95% CI) |
|
Composite Endpointa |
3.5% |
4.6% |
0.74 (0.60-0.92) |
|
Stroke |
1.1% |
1.7% |
0.67 (0.47-0.97) |
|
ACS |
1.3% |
1.9% |
0.67 (0.47-0.94) |
|
Acute Decompensated Heart Failure |
0.1% |
0.3% |
0.27 (0.08-0.98) |
|
Coronary revascularization |
0.5% |
0.7% |
0.69 (0.40-1.18) |
|
AF |
0.6% |
0.6% |
0.96 (0.55-1.68) |
|
CV Death |
1.6% |
1.5% |
1.11 (0.78-1.56) |
aStroke, ACS, acute decompensated heart failure, coronary revascularization, AF, or CV death.
Lloyd-Jones said the absolute reduction in the primary composite endpoint is clinically meaningful, translating into a number needed to treat (NNT) of about 90, which is lower than the NNT of 61 observed in SPRINT but “within the range of the other things we do for prevention very definitely.” He noted that the risk profile of participants in the STEP trial was generally lower than that of the SPRINT participants.
In terms of safety, Lloyd-Jones said “it’s very reassuring that they did not see substantial differences nor even substantial event rates in terms of kidney problems, falls, fractures, those sorts of things. So I think this tells us that in the majority of patients, we should be shooting for these lower blood pressure targets, as suggested in the American guidelines. Let’s get people to less than 130 if at all possible, of course monitoring them along the way to make sure they’re tolerating it.”
‘Bespoke Medicine’ for Older Adults
Commenting for TCTMD, Athanase Benetos, MD, PhD (CHRU de Nancy, University of Lorraine, France), agreed with Lloyd-Jones that STEP confirms the results of the SPRINT study. But Benetos, who specializes in geriatric cardiology, said that it doesn’t really answer the important question about what to do in elderly patients who are struggling with loss of function, loss of autonomy, and the burden of multiple medications, noting that the mean age in the trial was actually a bit lower than that in SPRINT (66 vs 68).
It remains unknown how best to treat patients older than 75 or 80, particularly those with frailty, cognitive decline, and serious comorbidities that would have precluded them from the randomized trials, he said. To help address this gap, he and his colleagues are running the RETREAT-FRAIL trial, which is assessing whether frail nursing home residents older than 80 who have low BP—which could be related to worse clinical outcomes in this population according to observational data—would benefit from less-intensive treatment. Results are expected in roughly 2-and-a-half years.
The overarching message is that it’s important to take each individual patient’s characteristics into account when selecting a treatment plan, Benetos advised. “Age is important, because age often is associated with these kind of problems of functionality, autonomy, and so on. But it’s not all about age. It’s very important to fix strategies according to the functional status, according to the autonomy status, according to several other medical issues before treating for years and years.”
Discussing the STEP results after Cai’s presentation, Bryan Williams, MD (University College London, England), one of the chairs of the European hypertension guidelines, agreed with this approach in older patients, who often have impaired baroreceptor function, stiff arteries, critical stenoses in arteries feeding vital organs susceptible to pressure reduction, and poor kidney function. As age increases, patient heterogeneity increases, too, such that at the same age, some people will be frail and dependent on care and others will be active and independent, Williams said.
“I think the elderly or the older population, when we’re treating blood pressure, is a classic example where we need not just guidance but actually some clinical decision-making on a patient-by-patient basis—bespoke medicine—with tailored blood pressure targets,” Williams said. “Perhaps as a consequence of this study, we could say that tailored targets in older patients over the age of 65 would be firstly, let’s try and get blood pressure below 140/90, because many patients never achieve even that level of control. And then aim to go lower down below 130 if you can and in those who will tolerate it, accepting that this is most likely to be possible in those who are independent, active, and less frail like in [STEP], and with fewer comorbidities.
“It’s not going to be easy to get there in everybody,” he continued, “and we should just try and get blood pressure as low as we can bearing in mind that tolerability is important in determining persistence with therapy.”

Todd Neale is the Associate News Editor for TCTMD and a Senior Medical Journalist. He got his start in journalism at …
Read Full BioSources
Zhang W, Zhang S, Deng Y, et al. Trial of intensive blood-pressure control in older patients with hypertension. N Engl J Med. 2021
Disclosures
- The trial was supported by grants from the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences, the Beijing Outstanding Young Scientist Program, and the National Natural Science Foundation of China. Olmesartan medoxomil tablets were donated by Nanjing Chia Tai Tianqing Pharmaceutical Company, amlodipine besylate tablets were donated by China Resources Saike Pharmaceutical Company, and BP monitors were donated by Omron Healthcare.
- The trial was supported by grants from the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences, the Beijing Outstanding Young Scientist Program, and the National Natural Science Foundation of China. Olmesartan medoxomil tablets were donated by Nanjing Chia Tai Tianqing Pharmaceutical Company, amlodipine besylate tablets were donated by China Resources Saike Pharmaceutical Company, and BP monitors were donated by Omron Healthcare. Cai reports no relevant conflicts of interest.
Related News

Comments