Better Hemodynamics, Less Mismatch With Self-Expanding TAVR vs Surgery
Effects were particularly marked in small annuli, although experts caution the impact on late outcomes is unknown.

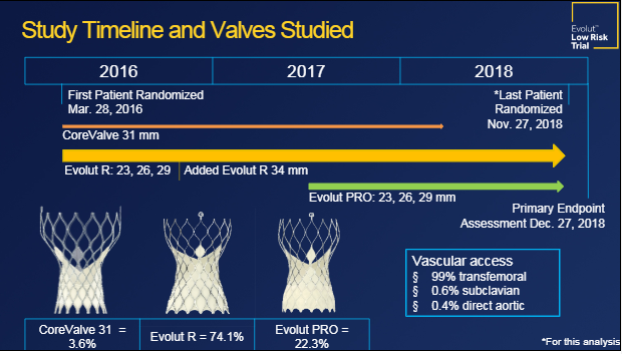
CHICAGO, IL—Patients undergoing TAVR with a self-expanding supra-annular bioprothesis (CoreValve, Evolut R, or Evolut PRO; Medtronic) have lower aortic valve mean pressure gradients, larger effective orifice areas, and less patient-prosthesis mismatch than patients treated with a surgical valve across a range of aortic annulus sizes, according to a new analysis of the Evolut Low-Risk Trial.
The largest advantages for TAVR were observed in patients with the smallest annuli, researchers reported recently at TVT 2019.
“Intrinsically, TAVR valves are considered to be better hemodynamically and our data showed that these patients did significantly better in terms of hemodynamics across all annular sizes, whether it was a big or small annular size,” lead investigator Mubashir Mumtaz, MD (University of Pittsburgh Medical Center/Pinnacle Health, PA), told TCTMD. “The differences were more remarkable in the small annuli, where we typically see patient-prosthesis mismatch or higher aortic valve gradients in surgical patients.”
Following surgery, patient-prosthesis mismatch—where the implanted aortic valve has an effective orifice area less than the native valve—has been linked with adverse clinical outcomes including mortality, rehospitalizations, decreased exercise capacity, and a higher rate of valve deterioration. At present, less is known about the clinical impact of patient-prosthesis mismatch following TAVR. Previous studies, including analyses of data from the CoreValve US Pivotal High-Risk trial, showed that annular size had a significant impact on valve hemodynamics and patient-prosthesis mismatch in SAVR subjects but not among those treated with TAVR. Also, TAVR was associated with better hemodynamics and less patient-prosthesis mismatch in patients with smaller annulus sizes (< 26 mm).
“As we’re moving into the lower-risk category—and these are the vast majority of patients with aortic stenosis who need treatment, who would have received aortic valve surgery in the past—if we’re going to offer them an alternative therapy that is equally good or superior to surgery, and much less invasive, then we need to make sure these patients do well over a long period of time,” said Mumtaz.
Small Annuli Implications in Surgery
In the present study, which Mumtaz presented at TVT 2019, patient-prosthesis mismatch was defined by effective orifice area adjusted for obesity, as recommended by the VARC-2 criteria. A moderate increase in the mean aortic valve gradient was defined as a 12-20 mm Hg rise at 30 days and a severe increase as a rise greater than 20 mm Hg. Using multislice CT, annular valves sizes were classified as small (< 23 mm), medium (23 to ≤ 26 mm or less), or large (> 26 mm).
Aortic valve mean gradient was significantly lower with TAVR than with surgery at 1 month (8.4 vs 10.5 mm Hg, respectively) and 12 months (8.6 vs 11.2 mm Hg, respectively), and the effective orifice area was significantly larger at 1 month (2.0 vs 2.2 cm2) and 12 months (2.3 vs 2.0 cm2). There was a consistent improvement in hemodynamics among patients with small, medium, and large annuli, but the difference between TAVR and surgery was most pronounced in those with small annuli, said Mumtaz.
At 30 days, there was significantly less moderate/severe patient-prosthesis mismatch in the TAVR arm. Stratified by annulus size, there was a “stepwise increase” in patient-prosthesis mismatch as annular sizes decreased in the surgical arm, but there was no correlation between annulus size and patient-prothesis mismatch in the TAVR-treated patients. In a comparison between TAVR- and SAVR-treated patients with small annuli, there was a significantly increased risk of patient-prosthesis mismatch at 30 days in the surgical arm.
Similarly, there was a stepwise increase in mean aortic valve gradient at 30 days as annular sizes decreased in the surgical arm, but no correlation between annulus size and aortic gradient in the TAVR arm. In patients with small annuli, aortic valve gradients were significantly larger in the surgical arm than in the TAVR-treated patients.
Long-term Follow-up Required
One of the limitations of their analysis is incomplete follow-up on the 1,402 patients. The primary endpoint was assessed when 850 patients reached 1-year follow-up and full echocardiographic results won’t be available until December. As a result, investigators were unable to assess the clinical and functional implications of patient-prosthesis mismatch. Additionally, the sample sizes within the small, medium, and large annuli groups were too small to assess clinical outcomes of those with and without mismatch.
To TCTMD, Mumtaz said there are data from the surgical field, including meta-analyses and retrospective studies, showing that patient-prosthesis mismatch and higher aortic valve gradients are associated with higher cardiovascular mortality and morbidity. “So TAVR valves, the way they’re designed with having less incidence of [patient-prosthesis mismatch] might be better in these low-risk patients,” said Mumtaz. “The hope is that this might correlate with better clinical outcomes in the long term. We don’t know that yet, but that’s why we’re following these patients.”
Martin Leon, MD (NewYork-Presbyterian/Columbia University Irving Medical Center, New York, NY), one of the session moderators, said the correlation between patient-prosthesis mismatch and clinical outcomes will be important, but he added it might be difficult to show this in the low-risk patient population. “It might take 2 or 5 years before you see that relationship unfold,” said Leon.
I think surgeons are underrecognizing this problem. Tsuyoshi Kaneko
Speaking during the session, panelist Tsuyoshi Kaneko, MD (Brigham and Women’s Hospital, Boston, MA), expressed surprise that 10.2% of patients with a small aortic annulus treated surgically have severe patient-prosthesis mismatch at 30 days. “I think surgeons are underrecognizing this problem,” said Kaneko, noting that as patients live longer its implications may become clinically apparent. “Occasionally, we’ll see in clinic a patient with a small valve who never really recovers from their symptoms,” he said.
In the Evolut Low-Risk Study, one-third of patients were treated with a sutureless surgical valve, which might have even lowered the incidence of patient-prosthesis mismatch in the SAVR group, said Mumtaz. However, in multivariate analysis, use of sutureless valves in the surgical arm was not a significant predictor of patient-prosthesis mismatch, he added.
Different Findings With Balloon-Expandable TAVR
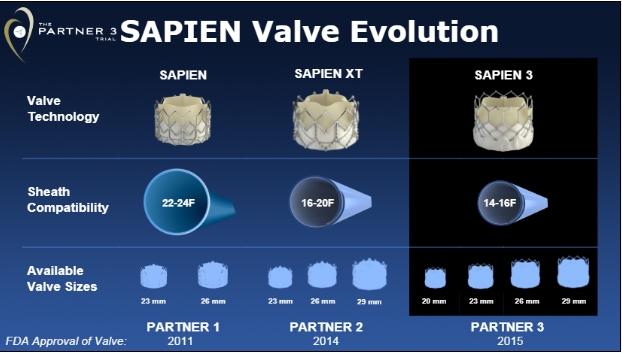
During the same late-breaking clinical trials session, Philippe Pibarot, PhD (Laval University, Quebec City, Canada), presented an echocardiographic analysis from the PARTNER 3 low-risk trial with the Sapien 3 device (Edwards Lifesciences). As reported previously, the balloon-expandable bioprothesis was associated with a higher mean aortic valve gradient and lower mean aortic valve area compared with surgery.
At 30 days, there was no significant difference in the incidence of severe or moderate patient-prosthesis mismatch between the TAVR and SAVR study arms, but the rate of mild and mild-to-moderate paravalvular aortic regurgitation was higher at 30 days and 1 year with TAVR. At 1 year, however, there was no significant association between early paravalvular aortic regurgitation and the risk of death, stroke, or rehospitalization at 1 year. Similarly, there was no association between patient-prosthesis mismatch or high residual aortic gradients and clinical outcomes at 1 year.
In contrast, a low-flow state (stroke volume index < 35 ml/m2) and impaired measures of right ventricular function at 30 days were associated with a higher risk of death, stroke, or rehospitalization at 1 year, said Pibarot. Like members of the panel, however, he agreed that longer-term assessment of clinical outcomes is required given the low baseline risk of patients in PARTNER 3.
Photo Credit: Pibarot P. Echocardiographic results of transcatheter versus surgical aortic valve replacement in low-risk patients: the PARTNER 3 trial. Presented at: TVT 2019. June 14, 2019. Chicago, IL.

Michael O’Riordan is the Managing Editor for TCTMD. He completed his undergraduate degrees at Queen’s University in Kingston, ON, and…
Read Full BioSources
Mumtaz MA. Hemodynamic outcomes and predictors of prosthesis-patient mismatch after transcatheter or surgical aortic valve replacement in low-risk patients: results from the Evolut R Low Risk Trial. Presented at: TVT 2019. June 14, 2019. Chicago, IL.
Pibarot P. Echocardiographic results of transcatheter versus surgical aortic valve replacement in low-risk patients: the PARTNER 3 trial. Presented at: TVT 2019. June 14, 2019. Chicago, IL.
Disclosures
- Mumtaz reports consulting for Abbott, Atricure, Medtronic, Z-media, JOMDD, and Terumo.
- Pibarot reports research support from and/or consulting for Edwards Lifesciences, Medtronic, Cardiac Phoenix, and V-Wave.
Comments