CT Scans Before and After TAVR Show Tricuspid, Bicuspid Valves Are Reassuringly Similar
A new imaging study hints that type 1 bicuspid disease is similar to tricuspid aortic stenosis in important and unexpected ways.

LONDON, England—There are more positive signs that current-generation transcatheter valves, originally designed to treat tricuspid aortic stenosis (AS), do just fine in the setting of bicuspid disease. A comparison of CT angiograms performed pre-and postimplantation suggests that the most commonly used TAVR devices appear to reshape the aortic annulus to the same degree in patients with bicuspid disease as they do in patients with tricuspid valves.
Didier Tchétché, MD (Clinique Pasteur, Toulouse, France), presented the results from the BAVARD multicenter register at PCR London Valves earlier this week.
This BAVARD analysis only looked at imaging results, Tchétché stressed in an interview with TCTMD. But he pointed out that these same patients are the ones being tracked in other registries that have considered outcomes such as paravalvular leak, stroke, bleeding, pacemaker implantations, etc, showing for the most part similar clinical outcomes between tricuspid and bicuspid valves.
In the current analysis, Tchétché and colleagues reviewed pre- and postimplantation CT scans for 97 patients with aortic bicuspid valve disease and compared these with 88 tricuspid AS patients. A total of 11 European centers contributed imaging data for the registry and most of the patients (92%) had type 1 bicuspid disease—the most common type seen among people of European descent. The TAVR devices most commonly used in Europe—Sapien 3 (Edwards Lifesciences), Evolut R (Medtronic), and Lotus (Boston Scientific)—were included in the analysis.
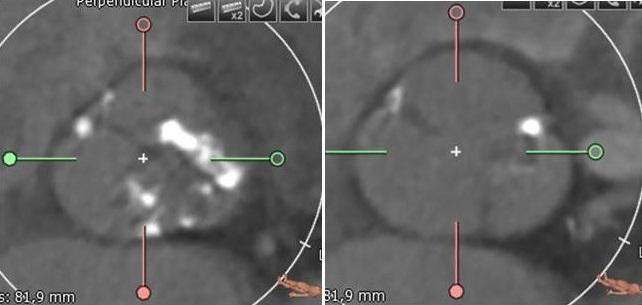
CT measurements of the annular diameter and intercommissural distance at baseline were roughly similar between the tricuspid and bicuspid groups, with intercommissural distance in bicuspid patients typically measured 4 mm above the level of the annulus. Mean annulus size was also different between the two groups: 23.6 mm for tricuspid AS patients and 26.9 mm for bicuspid AS patients.
Yet measurements gauged at assessing the ellipticity of the valve annuli at baseline were no different between the bicuspid and tricuspid groups. “We have had the feeling that bicuspid patients have a more elliptically shaped annulus—this is wrong, or it was not true in our registry. The annulus shape in both bicuspid and tricuspid patients is exactly the same, although the annulus for bicuspid patients is bigger at baseline,” Tchétché said. Measurements taken at different points along the cylindrical section of all three devices suggested that this was true and consistent for all three valve types.
What’s noteworthy, he continued, is that the ellipticity index for both types of valve disease was also similar postimplantation. “This is extremely important,” he said. “This shows that both devices reshape the annulus postimplantation—the circularity is the same. This is something new. We had the feeling that we might have more ellipticity in bicuspid patients postimplantation, but in fact, that’s not true.”
Another assumption has been that transcatheter valves are typically implanted at a different height in bicuspid patients, potentially increasing the risk of conduction system disturbances. In fact, said Tchétché, implantation depth was 3.4 mm in both the tricuspid and bicuspid group. “We had the feeling that we were implanting quite high, but in fact, we implant the devices exactly the same way in bicuspid and tricuspid patients,” he explained.
Finally, sizing of devices in both groups also appeared to be consistent with recommendations set out by device manufacturers for tricuspid AS, although final transcatheter heart valve diameter is typically dictated by the annular dimensions in the tricuspid patients and by the intercommissural distance in the bicuspid patients.
“Based on our study, we can say that second-generation devices, in general, work well in bicuspid patients,” Tchétché concluded, calling into question the need for dedicated bicuspid devices, something first contemplated when bicuspid disease patients were excluded from the early TAVR trials. At least for the type 1 bicuspid disease that made up the bulk of cases in this study, “I don’t think we need a dedicated device—the ones we have now are extremely efficient,” he said.
Jonathan Byrne, MD (King’s College Hospital, London, England), one of the session chairs, called the study “illuminating and intriguing” but pointed out that longer-term data will be necessary to confirm that any distortion to the annulus doesn’t end up having an impact on device durability over time. “We should be careful about extrapolating the results when we still wonder about the durability of a device that’s constrained at the leaflet tips over time, . . . even if you get a good acute result.”
Tchétché, agreeing that outcomes should continue to be tracked in patients with bicuspid disease, pointed out that ellipticity index was actually no different at baseline in the two groups. “It’s reassuring,” he said. “We can assume that if these devices work in tricuspid patients, there is no reason they won’t work in bicuspid patients as well.”
Also speaking with TCTMD, Ganesh Manoharan, MD (Royal Victoria Hospital, Belfast, Ireland), called the ellipticity observations the “most important finding” of the study.
“Despite what we previously thought about the elliptical nature of these valves, at least with these type 0 and type 1 bicuspid valves, it seems they can become circular, so whatever happens in the funnel, it can stretch to suit what’s happening at the annulus,” he explained.
There has also been research suggesting that TAVR devices need to be undersized in the setting of bicuspid disease, something that was not borne out in this analysis. “What this study supports,” Manoharan said, “is that you should size the device to the annulus just as you would a tricuspid valve, because whatever happens above will confirm to what is at the bottom. That’s important.”
Photo Credit: Didier Tchétché, adapted from: Expert Commentary: TAVR Device Selection and CT Sizing for Bicuspid Aortic Valves. TVT 2017

Shelley Wood was the Editor-in-Chief of TCTMD and the Editorial Director at the Cardiovascular Research Foundation (CRF) from October 2015…
Read Full BioSources
Tchétché D. Bicuspid aortic valve anatomy and relationship with devices. The BAVARD multicenter registry. Presented at: PCR London Valves 2017. September 25, 2017. London, England.
Disclosures
- Tchétché reports receiving honoraria or consultation fees from Medtronic, Edwards Lifesciences, Boston Scientific, Abbott Vascular, and 4Tech.
Comments