Expert Consensus Aims to Promote Cardiac CT Use in Preprocedural LAA Occlusion
Already “gold standard” for TAVR, cardiac CT holds advantages over TEE in this more complex anatomical structure, experts say.

An international group of experts is advocating for the use of CT as standard of care for preprocedural imaging in patients with A-fib undergoing left atrial appendage occlusion (LAAO) for the prevention of stroke.
The new consensus document, which was published online this week in JACC: Cardiovascular Interventions, outlines protocols for image preparation, acquisition, and interpretation.
“I'm very excited that we have this expert consensus document in print. It's extremely important, and it validates the role of CT in left atrial appendage planning,” Dee Dee Wang, MD (Henry Ford Health System, Detroit, MI), who served on the writing committee, told TCTMD. “It finally justifies what we've been demonstrating in the scientific research that the left atrial appendage is equally as important as an aortic valve replacement therapy and it requires this degree of planning by CT to make it a very safe procedure.”
CT is already the standard for preprocedural planning at most hospitals performing structural heart interventions, such as TAVR, said Wang. “Now it's just adapting that same CT scan and really just using the measurements for left atrial appendage, which in this paper we give different scenarios about how to really do it step-by-step and it's very simplistic,” she said. “The biggest challenge is overcoming the culture of change and realizing that it's okay to push the needle forward and it's okay to advance in the field.”
Why do we give the more complex anatomical structure less respect? Dee Dee Wang
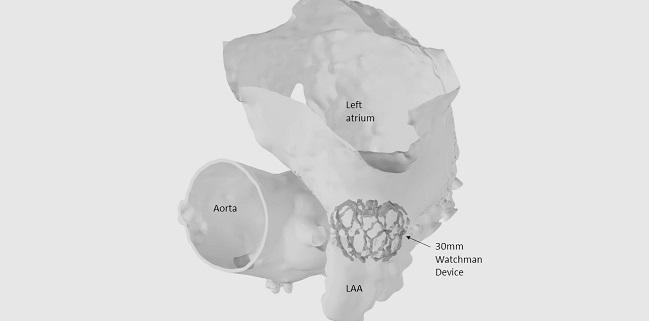
Wang likened the aorta to “just a tube,” while noting that the LAA is more complicated, “like a fingerprint.”
“Why do we use the less-sophisticated modality of imaging [for LAA occlusion] when there is one that will give us a consummate answer already available that we're using for a simpler structure?” she asked. “Why do we give the more complex anatomical structure less respect?”
Removing the Guesswork
Preprocedural CT is helpful in planning an LAA occlusion given the typically “complex, highly heterogeneous anatomy,” according to the authors. Preprocedural cardiac CT can help “to determine anatomical feasibility of the LAAO procedure, to provide accurate sizing of the LAA dimensions for device selection, periprocedural planning, and exclusion of LAA thrombus,” they write. “Additionally, 3-D volume rendering provides a roadmap for transseptal puncture and optimal C-arm angulations for device implantation, which may reduce the amount of contrast used during the procedure.”
In terms of patient preparation, noninvasive cardiac CT is associated with a greater degree of patient comfort compared with transesophageal echocardiography (TEE), which has been the standard of care. Proper patient hydration is key to optimal image acquisition, the authors stress. They also lay out the proper technical protocols with regard to ECG gating, acquisition techniques, and contrast injection depending on the scanner used.
Sameer Gafoor, MD (Swedish Heart and Vascular Institute, Seattle, WA), who was not involved with the consensus statement’s creation, is pleased with the new guidance. “It is always wonderful to have a group of people with this level of experience come together to create a best practices pathway for centers that are starting as well as trying to improve their own CT acquisition protocols for this technology,” he told TCTMD.
Additional imaging of the LAA can only help with procedural planning, but Gafoor noted that CT imaging is complex and requires best practices to achieve good images.
“CT imaging for LAAO is not something you can just put an order in and watch it come to real time and then go forward from that,” he said. “There's a lot of levers and pulleys and gears that are happening behind the scenes that makes this whole thing work. Whether it's a matter of making sure that the proper gating is done, whether it's a matter of making sure that the correct minimum slices are used, whether it's the patient preparation, the amount of water that's taken to make sure that patients aren't dehydrated—all of these affect our CT imaging and therefore will affect our outcomes.”
CT is going to be one of the powerhouses that every single structural program is definitely using for other structural heart procedures, so this is a natural progression in that direction. Sameer Gafoor
Wang stressed that TEE should not be fully tossed aside. “We still need TEE in the procedure to help guide the transseptal puncture and guide the actual procedure when it's being performed,” she said. However, CT safely and efficiently eases the planning of procedures by eliminating the variability among operators performing TEE for sizing purposes. “It gives operators the confidence about not only what device size to use for that specific patient but also what catheter to use for that patient's specific anatomy,” Wang explained. “And it gives the team a road map and a plan without having to figure it out on the table, which for 2019 should be the standard of care.”
Gafoor agreed that CT should be standard for preprocedural LAA occlusion planning going forward. “We need this process to be as turnkey as TAVR CTA protocols are because eventually this may come that we may think about moving away from transesophageal echocardiography altogether,” he said. “If we get to the point that we're starting to think about intracardiac echo [ICE] as a standard for left atrial appendage occlusion then proper CT done ahead of time helps us get there. That combination of CT and ICE is extremely powerful.”
However, the lack of standardized protocols and correlation of measurements with hard outcomes so far have been hurdles to widespread adoption of cardiac CT in this space, Gafoor commented, adding that this paper and potentially future ones addressing postprocedural evaluation will help. “CT is going to be one of the powerhouses that every single structural program is definitely using for other structural heart procedures, so this is a natural progression in that direction,” he predicted.
Photo Credit: Dee Dee Wang

Yael L. Maxwell is Senior Medical Journalist for TCTMD and Section Editor of TCTMD's Fellows Forum. She served as the inaugural…
Read Full BioSources
Korsholm K, Berti S, Iriart X, et al. Expert recommendations on cardiac computed tomography for planning transcatheter left atrial appendage occlusion. J Am Coll Cardiol Interv. 2019;Epub ahead of print.
Disclosures
- Korsholm reports receiving speaker's honorarium from Abbott.
- Wang reports receiving research grant support from Boston Scientific and serving as a consultant for Edwards Lifesciences, Boston Scientific, and Materialise.
Comments