Fivefold Increase in Impella Use for Cardiogenic Shock in Acute MI: US Data
The observational data also hint at higher in-hospital mortality compared with IABP, but only an RCT can rule out confounders.


Use of the Impella percutaneous left ventricular assist device (Abiomed) in acute MI complicated by cardiogenic shock (AMICS) in the United States increased nearly fivefold between 2012 and 2017, a retrospective analysis of the National Inpatient Sample (NIS) shows.
Moreover, compared with intra-aortic balloon pump (IABP) use, Impella was associated with higher in-hospital mortality and a greater need for transfusion.
Like other observational studies that have come before it, however, the current one—published in Catheterization and Cardiovascular Interventions—cannot rule out confounders since the choice of hemodynamic support strategy in this challenging scenario may have been influenced by multiple unknown factors, the authors warn. Their findings “underscore the need for rigorous, large-scale prospective clinical trials in AMICS patients to evaluate the safety and efficacy of Impella implantation,” urge Yeunjung Kim, MD (Yale University School of Medicine, New Haven, CT), and colleagues.
“In this retrospective study with use of Impella compared to IABP, we showed similar findings to prior studies of a mortality signal in use of Impella; however, despite propensity-matching, from administrative claims data it is difficult to understand whether confounders are at play,” senior author S. Elissa Altin, MD (Yale University School of Medicine), told TCTMD in an email. “For example, we cannot know when the IABP or Impella was placed during the hospitalization and in what stage of shock, [and] we cannot directly compare the hemodynamics, lab value assessments of hypoperfusion, severity of CAD, and success of revascularization between the study groups.”
Commenting for TCTMD, Srihari S. Naidu, MD (Westchester Medical Center, Valhalla, NY), also urged caution: “This kind of observational analysis, when you take a very high-risk population like cardiogenic shock, is going to be fraught with significant confounders that can’t be evaluated in the context of any type of adjusted analysis, including propensity matching.”
For example, academic medical centers are more apt to use Impella and on the whole tend to treat sicker patients than do smaller community hospitals. “So by definition you’re going to get a selection bias or a referral bias, where Impella patients are also the sicker patients,” he observed.
Trends Across 6 Years
Kim, Altin, and colleagues used the NIS data set to identify 54,480 hospitalizations for AMICS that involved Impella or IABP support between 2012 and 2017. Patients who received both devices were excluded.
Overall, 10.6% of the cases used Impella, but the proportion increased yearly over the study period—rising nearly fivefold from 4.1% in 2012 to 19.9% in 2017 (P for trend < 0.01). “MCS device utilization increased in all regions of the United States except the Northeast. The greatest increase occurred in the Southern region,” the researchers note, adding, “Impella use over the study period accelerated most in patients who were younger with fewer comorbidities.”
Baseline demographic factors (age, sex, race) were similar irrespective of MCS type. However, the Impella patients were less likely to have hypertension, hyperlipidemia, CAD, chronic obstructive pulmonary disease, congestive heart failure, and atrial fibrillation, whereas they were more apt to have PAD. At the hospital level, larger centers were more likely than small- and medium-sized centers to use Impella versus IABP.
The researchers performed propensity-score matching that accounted for age, sex, and comorbidities as well as other variables like presence of STEMI or cardiac arrest, need for cardiopulmonary resuscitation, use of PCI, obesity, and blood loss, among others. This resulted in 5,750 matched pairs.
Compared with IABP, Impella use was linked to higher in-hospital mortality (OR 1.74; 95% CI 1.41-2.13) and added risk of transfusion (OR 1.97; 95% CI 1.40-2.78). There were no differences in acute kidney injury or stroke. The data also point to significantly higher hospital costs with Impella (mean difference $22,416.80; 95% CI $17,029-$27,804).
That costs rose in conjunction with more devices comes as no surprise, Kim and colleagues say, but the association between the type of hemodynamic support and outcomes is less conclusive.
“Although our data showed a trend toward increased mortality with Impella versus IABP, this may well have been predominantly a function of case selection wherein sicker patients received Impella support. The intrinsic methodological limitations of the present study preclude firm conclusion whether this mortality observation reflects patient selection or actual contributions of device complications,” they say.
SCAI Update Forthcoming
Naidu, along with Ankur Kalra, MD (Cleveland Clinic, OH), led a similar study a few years back that leveraged the NIS data, though they cast a wider net by looking at not just Impella and IABP but also extracorporeal membrane oxygenation and nonpercutaneous left ventricular assist devices. Their data set also ended earlier, in 2015. “I think it’s interesting to note that within an additional 2 years of analysis . . . there was a significant rise in Impella utilization across the United States. That is kind of an inflection point,” Naidu observed.
He also drew attention to the regional patterns, proposing that increases were larger in the South because Impella use historically has been higher in the Northeast. “And so it’s catching up in different parts of the country,” Naidu said.
What would enable more-precise comparisons between Impella and IABP is the shock classification system developed by the Society for Cardiovascular Angiography and Interventions (SCAI), said Naidu, who chaired the group behind its creation.
“Even if you do these [propensity-matched] analyses, it’s very hard to know if in the Impella group and the balloon-pump group there were the same proportions of patients in the various shock categories,” he said. Two patients can have the same demographics, but one of them might be much sicker. Not adjusting for shock severity, stressed Naidu, “is a big problem.”
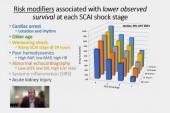
Altin agreed, pointing out that the SCAI definitions help clarify which patients are most at risk based on a combination of hemodynamic presentation, coronary anatomy, and key risk factors. “I see this study as building the knowledge base around AMICS,” she said. “In general, early revascularization is our best primary treatment of AMICS. Despite a proliferation of percutaneous mechanical circulatory support devices, mortality remains unacceptably high. Early identification of shock is important to management. The SCAI shock definitions are critically helpful in this regard,” and should be incorporated into administrative coding, she suggested.
“For example, ‘Impella insertion for Stage [ ] shock,’ ‘intubation for Stage [ ] shock.’ Since we rely on administrative data for retrospective analyses, we need to move beyond coding that is just useful for billing and rather more clinically descriptive,” Altin said. “Ultimately, AMICS is a moving target throughout a hospitalization and patients may present in stage A with rapid decompensation to stage D or vice versa after revascularization; however we don’t know the outcomes based on the trajectory of shock progression. Further understanding of this will likely inform subsequent therapies to improve mortality.”
Looking ahead, an update to the SCAI categories will be released in October, Naidu predicted. “That’s going to be a big deal, because it’s looking at all the data that we have accumulated in 2 years, which is about 13 or 14 different studies, and then reincorporating that into a better, more-granular, and more-robust . . . shock pyramid and classification scheme.”
For now, it’s not clear whether databases like NIS can effectively be used to “try to retrofit a shock stage,” Naidu noted. “It’s not clear that they have all the variables that we need to [do it].”
Naidu said a better approach would be, from the outset, to gather these variables consistently across different studies. Then researchers could focus on particular subsets of severity. “That makes a lot more sense, because now you have a narrow window of patients that you can then propensity match . . . in terms of age, race, gender, renal insufficiency, and whatnot,” he explained.
Prospective trials of MCS also could target particular categories, such as shock C and D, Naidu added. “That way you know what you’re getting, and all hospitals will have [both] Impella and balloon pump.”

Caitlin E. Cox is Executive Editor of TCTMD and Associate Director, Editorial Content at the Cardiovascular Research Foundation. She produces the…
Read Full BioSources
Kim Y, Shapero K, Ahn SS, et al. Outcomes of mechanical circulatory support for acute myocardial infarction complicated by cardiogenic shock. Catheter Cardiovasc Interv. 2021;Epub ahead of print.
Disclosures
- Kim, Altin, and Naidu report no relevant conflicts of interest.
Related News


Comments