Milrinone, Dobutamine Comparable for Cardiogenic Shock: DOREMI
The trial confirms that “we can go for the much cheaper dobutamine in this situation,” Holger Thiele says.

A head-to-head comparison of inotropes in the setting of cardiogenic shock revealed no clear victor, with milrinone and dobutamine providing similar outcomes in the randomized DOREMI trial.
A composite primary outcome event occurred in 49% of patients treated with milrinone and 54% of those treated with dobutamine, a nonsignificant difference (P = 0.47). There also were no differences for any secondary outcomes, including in-hospital mortality (37% vs 43%), or for any biochemical or hemodynamic parameters.
Thus, the choice of inotrope “comes down to is physicians’ preference and physicians’ comfort,” senior author Benjamin Hibbert, MD, PhD (University of Ottawa Heart Institute, Canada), told TCTMD. He added that cost is a consideration, too, noting that milrinone is “10 times” more expensive than dobutamine.
His center had been preferentially using milrinone for cardiogenic shock. “I now use dobutamine preferentially unless there’s something about the patient’s hemodynamic profile that makes me select milrinone,” Hibbert said, “although I recognize that that’s a bias and that as far as the data that we have available to us, there’s no important clinical differences. So still dealer’s choice.”
Commenting for TCTMD, Holger Thiele, MD (Heart Center Leipzig, Germany), pointed out that this is the first large-scale comparison of different inotropes in the setting of cardiogenic shock. “From this perspective, this is very good that we have more evidence on the possible best inotrope in this situation,” said Thiele.
But he added that he was surprised dobutamine was compared with milrinone, as the latter drug is rarely used for cardiogenic shock in Europe and is more commonly employed by cardiac surgeons as a bridge to transplant or implantation of an LV assist device.
Despite that issue and some other limitations, Thiele said, the trial results confirm recommendations in German/Austrian cardiogenic shock guidelines to preferentially use dobutamine. “So we do not need to use milrinone . . . and we can go for the much cheaper dobutamine in this situation,” he said.
The findings were published in the August 5, 2021, issue of the New England Journal of Medicine, with lead authors Rebecca Mathew, MD, and Pietro Di Santo, MD (both of the University of Ottawa Heart Institute).
DOREMI Trial
Hibbert told TCTMD that there is a common debate in CV medicine about whether milrinone or dobutamine is better in cardiogenic shock. His team performed a systematic review and meta-analysis to examine the data, “and we realized there’s really an evidence gap here,” he said, adding, “As mechanical circulatory support becomes more and more of a focus of shock management, it’s important to know if there are big differences in outcomes between the medical arms.”
People kind of felt that milrinone was better, and as with so many things in cardiogenic shock, this was a big swing and a miss. Benjamin Hibbert
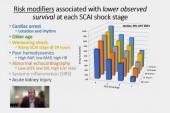
For the DOREMI trial, the investigators enrolled 192 patients with cardiogenic shock admitted to the cardiac ICU at their center between September 1, 2017, and May 17, 2020. Patients met Society for Cardiovascular Angiography & Interventions (SCAI) criteria for stage B, C, D, or E cardiogenic shock, although roughly 90% fell within stage C (“classic”) or stage D (“deteriorating”).
Patients in the two trial arms were well matched, with an average age of 69 to 72, while 35% to 38% of participants were women and 65% to 69% had ischemic cardiomyopathy. Median serum lactate level at baseline was elevated to 2.9 mmol/L in both groups.
The primary outcome was a composite of in-hospital death, resuscitated cardiac arrest, receipt of a cardiac transplant or mechanical circulatory support (MCS), nonfatal MI, TIA/stroke diagnosed by a neurologist, or initiation of renal replacement therapy. There was no difference in this outcome between the milrinone and dobutamine groups (RR 0.90; 95% CI 0.69-1.19). None of the individual components differed either.
Moreover, there were no significant differences in terms of the duration of inotropic treatment, length of stay in the ICU or hospital, need for noninvasive/invasive mechanical ventilation, duration of ventilation, arrhythmia requiring intervention, acute kidney injury, heart rate, mean arterial pressure, vasoactive-inotropic score, serum lactate level, serum creatinine level, or hourly urine output. Safety, reflected by rates of atrial or ventricular arrhythmias, sustained hypotension, or intensification of vasopressor therapy, was similar in both trial arms.
“People kind of felt that milrinone was better, and as with so many things in cardiogenic shock, this was a big swing and a miss,” Hibbert said. “And I think that’s just because with cardiogenic shock if you don’t have something to address the underlying cause that brought them into it, my bias is that it doesn’t really matter what we do for these patients. So if the ship’s sinking, rearranging the deck chairs doesn’t really drive a large [part of the] outcome.”
It will be important, then, to “address shock earlier so that we don’t get into the end-organ damage and multisystem failure,” he said. “And secondly, we’ve got to find things that address underlying causes of the cardiogenic shock. Otherwise, even if we resuscitate the patients, they slip back into shock once we discontinue these agents. So I think that the important differences that we thought we might see just don’t exist because we’re not addressing the underlying etiology of the shock.”
Some Limitations
Thiele pointed out some issues with the trial, including a sample size calculation based on a “very optimistic” 20% absolute reduction in risk with milrinone. Based on existing data, he said, “I would have never assumed that milrinone would lead to any significant benefit in comparison to dobutamine.” Whether there could be a smaller, but still clinically important, advantage for milrinone cannot be answered by this trial, he added.
The composite primary outcome is problematic as well, Thiele said, because some of the components represent competing risks or don’t make sense to include. For instance, there’s no reason to expect that milrinone would reduce stroke, he said. “So this looks like a very artificial combined clinical endpoint that they have chosen.”
In addition, the trial was conducted at a single center among a heterogeneous group of patients with cardiogenic shock, complicating interpretation, Thiele commented. Though the high rate of in-hospital mortality indicated that appropriate patients were selected, he said, “overall it was much too optimistic to find any benefit with milrinone in this setting with this combined clinical endpoint.”
Hibbert acknowledged some of these limitations, but said “it’s the best data we have right now.”
Since the results were published, several commentators have pointed out that the trial doesn’t address the fundamental question of whether inotropes as a whole are beneficial or harmful in cardiogenic shock, which has never been answered in a placebo-controlled trial.
To that end, Hibbert and his colleagues have designed a follow-up trial called DOREMI 2, which will be a placebo-controlled trial of inotropes versus placebo in the early resuscitative phase (the first 12 hours) of cardiogenic shock.

Todd Neale is the Associate News Editor for TCTMD and a Senior Medical Journalist. He got his start in journalism at …
Read Full BioSources
Mathew R, Di Santo P, Jung RG, et al. Milrinone as compared with dobutamine in the treatment of cardiogenic shock. N Engl J Med. 2021;385:516-525.
Disclosures
- The trial was funded by the Innovation Fund of the Alternative Funding Plan for the Academic Health Sciences Centres of Ontario.
- Di Santo, Hibbert, and Mathew report no relevant conflicts of interest.
Related News


Comments