MitraClip Viable in Shock Patients With Significant MR: Observational Study
The short-term results looked promising, and the time is right to test the device in a randomized trial, one expert says.


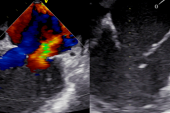
Patients in cardiogenic shock with significant mitral regurgitation (MR) appear to fare well in the short term when treated with transcatheter edge-to-edge repair (TEER), according to a new observational analysis.
The in-hospital mortality rate among those treated with MitraClip (Abbott) was 23%, with shock patients who presented with MR in the setting of acute MI faring worse than those without acute MI.
Published this week in JACC: Cardiovascular Interventions, Medhat Farwati, MD (Cleveland Clinic, OH), and colleagues say their data suggest that TEER with MitraClip may be a reasonable therapeutic option in this high-risk population with limited available treatments.
Benjamin Hibbert, MD, PhD (University of Ottawa Heart Institute, Canada), who wasn’t involved in the study but is part of the CAPITAL research group launching a randomized trial with MitraClip in shock patients, said this newest analysis “adds to the chorus of studies demonstrating the feasibility of TEER in patients with cardiogenic shock.” Operators are becoming increasingly more comfortable taking the sickest patients for a MitraClip procedure, he said, and “getting results that at first blush appear very encouraging.”
“To treat these patients and achieve an in-hospital mortality rate of 23% is impressive, and one would be tempted to conclude that TEER could account for this apparent reduction,” he said. While that conclusion would be tempting, it would also be too hasty, stressed Hibbert. “Of course, observational and/or administrative data doesn’t allow us to conclude this.”
Rodrigo Estévez-Loureiro, MD, PhD (University Hospital Alvaro Cunqueiro, Vigo, Spain), who led the IREMMI study, said the new paper is gratifying to see published because it provides reassurances about the use of MitraClip in shock patients with significant MR. “It’s minimally invasive, and there is a lot to win and very little to lose with the procedure,” he told TCTMD. “I think we should emphasize that the role of edge-to-edge repair MitraClip is becoming more predominant in these patients.”
Significant MR Complicated by Shock
There are two distinct types of cardiogenic shock patients who will present with severe MR, explained Estévez-Loureiro. The first group includes those with an ischemic or nonischemic cardiomyopathy who progress to end-stage heart failure and cardiogenic shock, while the second includes those who end up in cardiogenic shock following an acute event, such as STEMI. In the latter patients, MR might develop as a result of severe damage to the mitral valve, including complete or partial papillary muscle rupture.
Sometimes the ideal is different from what we can achieve in real life. Rodrigo Estévez-Loureiro
To date, there have been limited data on the use of MitraClip in patients with MR and cardiogenic shock. In the IREMMI study, presented last year at TCT Connect 2020, mortality at 30 days was 10% among those with cardiogenic shock who underwent TEER. At the same meeting, Hibbert presented patient-level data from a multicenter analysis of 141 patients in cardiogenic shock who had moderate-to-severe MR treated with MitraClip. Here, the in-hospital mortality was 15.6%.
In this latest study, the researchers identified 639 patients with significant MR who presented in cardiogenic shock and who underwent a MitraClip procedure during the same hospital admission. Patients were also stratified by the presence or absence of acute MI, with 179 and 460 patients presenting with and without acute MI, respectively. The median age of patients was 73 years, and this was similar among those with and without acute MI. Patients with acute MI were more likely to require mechanical circulatory support (MCS) and have a history of CAD.
While the overall in-hospital mortality rate was 23%, the rate was higher for shock patients with significant MR and acute MI (29.6%). The in-hospital mortality rate for those with both shock and MR but not acute MI was 20.4%.
In the multivariable analysis, predictors of mortality in the overall population included older age (OR 1.04 per 1-year increment; 95% CI 1.02-1.06), MCS use (OR 2.76; 95% CI 1.83-4.17), end-stage renal disease (OR 2.81; 95% CI 1.44-5.49), and obesity (OR 2.24; 95% CI 1.05-4.77). In patients with and without acute MI, the highest risk of death was observed in patients aged 75 to 84 years, while those younger than 65 were least likely to die during hospitalization.
In follow-up, the 30-day readmission rate was 26.3% in the overall cohort, with similar rates seen in those with and without acute MI.
To TCTMD, Estévez-Loureiro said the in-hospital mortality rate seen in the present study is in line with a real-world analysis he published earlier this year along with Gilbert Tang, MD, MBA (Mount Sinai Health System, New York, NY). In that study, use of MitraClip for cardiogenic shock patients increased over time and was associated with significantly lower risk of death compared with no TEER.
Time for a Randomized Trial
In their paper, the researchers say it’s not entirely clear why patients without acute MI fared better with MitraClip than those who presented with MR and cardiogenic shock following an acute MI. Use of MCS was lower in patients without acute MI, which “probably indicates a more favorable hemodynamic profile in the nonacute MI group and may result in improved survival,” write Farwati and colleagues.
To TCTMD, Hibbert said the comparison between patients with versus without acute MI is important because MI-associated shock patients tend to fare worse. For these patients, revascularization proceeds first, with operators waiting to see if the MR improves following PCI. If there is no improvement, the patient is brought back for a MitraClip procedure.
On the whole, Hibbert said the currently available evidence is insufficient to start implanting the MitraClip in patients with cardiogenic shock and significant MR. For example, in the latest analysis of ICD codes from Farwati and colleagues, the timing of TEER relative to cardiogenic shock is unclear. The shock patients treated with MitraClip might have been resuscitated, with TEER performed later in the hospital admission. As a result, indication bias might account for the lower rate of mortality, said Hibbert.
“Moreover, the lack of a comparison group of untreated [cardiogenic shock] patients prevents a meaningful comparison,” he said. “However, I sympathize with the authors. We similarly were asked to provide a comparison group in our analysis of patient-level data, and when we looked almost all the untreated patients were dead. There was clearly profound confounding that no amount of statistical wizardry would be able to adjust for.”
Hibbert thinks the time is right for a randomized controlled trial testing TEER in patients with MR complicated by cardiogenic shock, given the limited number of treatment options. Their upcoming trial, known as CAPITAL MINOS, will hopefully answer this important question, he said. In that study, they have mandated a minimum of 48 hours between revascularization for acute MI and TEER in order to see if MR improves before proceeding with the MitraClip.
On the other hand, Estévez-Loureiro said there are now several observational studies, including those with propensity matching, that show use of MitraClip reduces the risk of death compared with no TEER, and said these data can be used to guide practice. While it would be ideal to have randomized controlled trial results, such a study will be difficult to conduct.
“Sometimes the ideal is different from what we can achieve in real life,” Estévez-Loureiro said. “We have to use our observational data to guide us a little bit,” he added, noting that all patients should undergo a detailed evaluation from the heart team before any treatment course is decided upon.

Michael O’Riordan is the Managing Editor for TCTMD. He completed his undergraduate degrees at Queen’s University in Kingston, ON, and…
Read Full BioSources
Farwati M, Saad AM, Abushouk AI, et al. Short-term outcomes following urgent transcatheter edge-to-edge repair with MitraClip in cardiogenic shock: a population-based analysis. J Am Coll Cardiol Interv. 2021;Epub ahead of print.
Disclosures
- Hibbert reports funding for work as a clinical trial investigator from Abbott, Boston Scientific, and Edwards Lifesciences.
- Estévez-Loureiro reports consulting for Abbott and Boston Scientific.
Related News

Comments