More Conservative Antibiotic Prophylaxis for Infective Endocarditis Seems Safe, Appropriate
Rates of IE over time remained stable in California and New York, even as recommendations on antibiotic use became more restrictive.

Over a decade-and-a-half that saw major changes to guidelines for antibiotic prophylaxis, rates of infective endocarditis (IE) remained stable in California and New York, with some changes in patterns of patient characteristics and types of disease, a new analysis shows.
The observed lack of change in IE incidence between 1998 and 2013 is “really important” because there had been very few contemporary studies addressing the potential impact of the guideline changes, which restricted use of antibiotic prophylaxis, study author Joanna Chikwe, MD (Mount Sinai Medical Center, New York, NY), told TCTMD.
“Previously, we were much more liberal about recommending people take antibiotics to protect themselves from infective endocarditis and [the guideline writers] looked at a lot of data and basically decided that it’s actually reasonable that only high-risk patients take antibiotics,” she said.
Demonstrating that there was no spike in IE cases after the change in recommendations “means that fewer patients need to be exposed to antibiotics,” Chikwe continued. “You’re not risking antibiotic resistance, and you’re not exposing more people to a risk of what’s essentially a life-threatening illness.”
The American Heart Association revised its guidelines for IE prophylaxis in April 2007, and “the main changes were removal of the recommendations for routine antibiotic prophylaxis for invasive dental procedures in low- and moderate-risk patients and for most other invasive procedures in all patients,” the authors, led by Nana Toyoda, MD (Mount Sinai Medical Center), note, adding that recommendations from other organizations have similarly become more restrictive over time.
Prior studies have shown that the changes were associated with large declines in prescribing of antibiotic prophylaxis, but the evidence is mixed as to whether there has been an impact on IE incidence and mortality.
In this study, published in the April 25, 2017, issue of the Journal of the American Medical Association, the investigators explored that issue and others by examining data from mandatory statewide databases on 75,829 patients hospitalized with a first episode of IE in California or New York.
After adjustment for age, sex, and race, annual incidence of IE remained stable at 7.6 to 7.8 cases per 100,000 people throughout the study period. There was no signal of an increase in the rate after the major guideline changes in 2007.
The relative proportions of different types of IE did, however, shift between 1998 and 2013. There was a drop in the proportion of native-valve endocarditis (74.5% to 68.4%) and increases in the proportions of prosthetic-valve disease (12.0% to 13.8%) and cardiac device-related endocarditis (1.3% to 4.1%; P < 0.001 for all).
Healthcare-associated IE accounted for about half of cases throughout the study period, with a slight decrease in nosocomial disease accompanied by a slight increase in nonnosocomial IE. The proportion of patients on dialysis also rose, making up 35% of healthcare-associated cases at the end of the study period.
Mortality overall showed a small decline of 2% per year during the study period, but it remained higher with healthcare-associated versus community-acquired cases (adjusted HR 1.52; 95% CI 1.48-1.56). Chikwe attributed the improvement in outcomes to practice changes that result in earlier recognition of and intervention for IE.
There were some changes in the pathogens responsible for IE over time, but an increase in oral streptococcal disease—which might be expected with more restrictive use of prophylaxis for dental procedures—was not observed after the guideline changes.
“We’ve shown that a much more tailored and focused approach—just treating the high-risk patients that you have—is safe and appropriate,” Chikwe said.
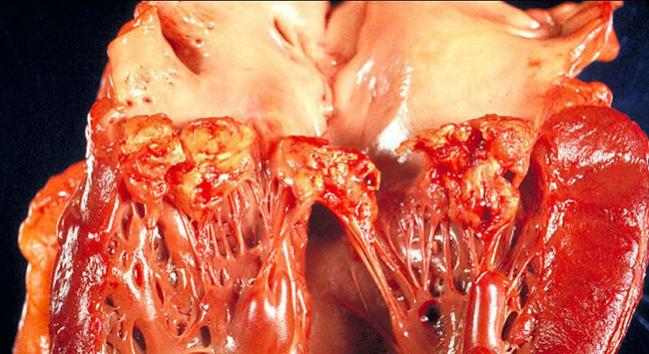
Photo Credit: US Centers for Disease Control and Prevention/Dr. Edwin P. Ewing Jr. As a work of the US federal government, the image is in the public domain.
{kind=link}

Todd Neale is the Associate News Editor for TCTMD and a Senior Medical Journalist. He got his start in journalism at …
Read Full BioSources
Toyoda N, Chikwe J, Itagaki S, et al. Trends in infective endocarditis in California and New York State, 1998-2013. JAMA. 2017;317:1652-1660.
Disclosures
- Toyoda reports receiving a research stipend from the Department of Cardiovascular Surgery, Icahn School of Medicine, Mount Sinai Medical Center.
- Chikwe reports receiving speaker honoraria from Edwards Lifesciences.
Comments