Optimizing Medical Therapy Before Clip Repair for MR? ‘This Is Hard’
Getting patients on max doses of guideline-directed heart failure therapies is important but also challenging, experts agree.


MIAMI, FL—A debate at TVT 2021 last week was supposed to be about whether guideline-directed medical therapy should be tried at maximally tolerated doses before patients undergo transcatheter edge-to-edge repair (TEER) for functional mitral regurgitation (MR), but it ended up focusing on the difficulty of getting patients on foundational heart failure therapies in the first place.
JoAnn Lindenfeld, MD (Vanderbilt Heart and Vascular Institute, Nashville, TN), led off by arguing that drug therapy should be maxed out first, but her ostensible opponent didn’t disagree.
“I want to concede the debate to JoAnn. I think she made a convincing argument, and I really don’t have much to add to what she said,” Milton Packer, MD (Baylor Heart and Vascular Institute, Houston, TX), said.
Instead, Packer spent his time arguing for a more-practical approach to initiating proven heart failure drugs like ACE inhibitors/ARBs, sacubitril-valsartan (Entresto; Novartis), beta-blockers, mineralocorticoid receptor antagonists (MRAs), and sodium-glucose cotransporter 2 (SGLT2) inhibitors, a time-consuming process that rarely results in patients getting target doses of all of the foundational therapies.
Talking about conventional sequencing of drug initiation, Packer said, “If you do this in a reasonably compulsive way, it will take 6 months. And people don’t do this.” Less than 5% of patients receive four foundational drugs at therapeutic doses, he added, underscoring a point made by Lindenfeld: major delays in starting these therapies lead to hospitalizations and deaths.
Clyde Yancy, MD (Northwestern Medicine, Chicago, IL), succinctly summed up the issue after Lindenfeld and Packer spoke: “In clinical practice this is really hard to do, and we need more implementation science to discover a new way to do this and better titration targets.”
Benefits of Medical Therapy
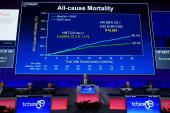
Lindenfeld laid the groundwork for her argument that medical therapy should be tried prior to edge-to-edge repair, but highlighted the benefits of having patients on all of the major drug classes. She pointed to 2020 study in the Lancet estimating that the addition of newer drugs like sacubitril/valsartan and SGLT2 inhibitors to ACE inhibitors/ARBs and beta-blockers would provide an 8-year boost in life expectancy for patients with heart failure and reduced ejection fraction.
The best option, I would conclude, is what was done in COAPT: maximally tolerated guideline-directed medical therapy first. JoAnn Lindenfeld
“So I don’t want us to underestimate here the benefit of guideline-directed medical therapy,” she said, noting that the benefits have been shown to occur very early in the pivotal trials. “If you delay this, for example, to do a procedure, [then] you delay substantial benefits. TEER is great, but medical therapy is pretty good, too, even early on.”
Unfortunately, most patients never see the full benefits of these drugs. A 2018 analysis of the CHAMP-HF registry, Lindenfeld pointed out, showed that many—and sometimes most—patients without contraindications were not treated with the foundational therapies and that less than 1% were receiving target doses of all of them. “If you’re referred an undertreated patient, you do a procedure, and you send them back, they’re likely to still be undertreated and you maybe lose 8 years of life,” she stressed.
Even within the COAPT trial, which established the benefit of TEER with the MitraClip (Abbott) for patients with functional MR, those who had their MR reduced to 2+ or less derived similar benefits, regardless of whether it was achieved with the device or optimal medical therapy alone, Lindenfeld said. And another analysis of 63 patients referred for a MitraClip procedure, most of whom had 3 to 4+ functional MR, showed that 57% no longer had MR that severe after receipt of the foundational heart failure therapies and thus “no longer had indications for TEER,” she said.
Lindenfeld also highlighted data indicating how difficult it can be to select individual patients who might benefit most from medical therapy. “So the best option, I would conclude, is what was done in COAPT: maximally tolerated guideline-directed medical therapy first,” she said.
Getting Treatment Started Quickly
Acknowledging the importance of the foundational heart failure therapies, Packer discussed the rationale behind a rapid-sequencing approach he’s proposed along with John McMurray, MD (University of Glasgow, Scotland). Instead of the process taking 6 months, it would take 4 weeks: start with beta-blockers and SGLT2 inhibitors, add sacubitril/valsartan 2 weeks later, and then add an MRA 2 weeks after that.
This strategy takes into account data showing that the order in which these drugs are started doesn’t affect their clinical benefits, although it can affect their safety. Hypotension and azotemia related to ACE inhibitors, for instance, can be mitigated by diuretics, which are also important for preventing early worsening of heart failure seen with beta-blockers, Packer pointed out. And there is evidence that MRA-related hyperkalemia can be reduced by a neprilysin or SGLT2 inhibitor.
Rapid sequencing also is supported by data from the pivotal trials themselves, which show that in the early stages—when treatments are being uptitrated to target doses—there are still substantial benefits from active treatment relative to placebo.
“Low starting doses of foundational drugs have very meaningful effects, so broad-based coverage should be prioritized before uptitration,” Packer concluded “People should be on all four classes of drugs within 4 weeks of initiation of therapy. I agree with JoAnn. Time is of the essence.”
‘75% of the Time There’s a Big Miss’
In his comments, Yancy said the “more-telling” data point from the CHAMP-HF registry was that only 25% of patients were on any dose of any medication from each of the foundational drug classes. “That tells us that in sophisticated practices, 75% of the time there’s a big miss. In my own practice, I have to be super diligent to make this happen. It takes a lot of time and effort, and I’m not certain [it] can be applied outside of a major academic medical center with the care team that’s involved. So the most important takeaway is that this is hard.”
I think sometimes people get distracted by the MR and forget that there’s a patient with ventricular disease that benefits from these medications. Paul Grayburn
One of the issues is that approaches to starting patients on these therapies is based on empiricism, without any guidance from biological studies, according to Yancy. Moreover, “this is a very draconian approach,” he said. “You titrate and titrate until you hit the max tolerable dose. Let’s be clear: that means the patient’s mental function is changing or the patient’s blood pressure is changing. There should be a more sophisticated way. Perhaps that answer is in biomarkers, but we should have a better surrogate marker of the adequacy of these therapies.” Expecting all patients to respond the same regardless of age, body size, and demographic background, too, “gives me a little bit of pause,” Yancy added.
Gregg Stone, MD (Icahn School of Medicine at Mount Sinai, New York, NY), raised a provocative question during a panel discussion, acknowledging the difficulty of getting patients on maximally tolerated doses of the major heart failure drugs: Does that argue for earlier consideration of TEER to treat MR?
“I’m not so sure, no,” Mayra Guerrero, MD (Mayo Clinic, Rochester, MN), said. “I think that we need to start with medications.” If patients get referred for TEER and aren’t taking even basic medications, they’ll get referred to a heart failure specialist first, Guerrero noted.
Paul Grayburn, MD (Baylor Scott & White Health, Dallas, TX), commented that it is a mistake to oversimplify functional MR, as it’s a “spectrum of very different diseases.”
But, he continued, “having said that, I think JoAnn made that key point . . . that you can add 8 years of people’s life by treating them with appropriate medicines in heart failure. So to some extent we should forget about MR for a minute and say are we treating the heart failure, the left ventricle of the patient, right? And if there is MR, where does MitraClip fit into that? But I think sometimes people get distracted by the MR and forget that there’s a patient with ventricular disease that benefits from these medications.”

Todd Neale is the Associate News Editor for TCTMD and a Senior Medical Journalist. He got his start in journalism at …
Read Full BioSources
Multiple presentations. TVT 2021. July 20, 2021. Miami, FL.
Disclosures
- Lindenfeld reports consulting fees/honoraria/speaking fees from Abbott Vascular, AstraZeneca, Boehringer Ingelheim, Boston Scientific, CVRx, Edwards Lifesciences, Impulse Dynamics, St. Jude Medical, and V-Wave, as well as institutional grant support/research contracts from AstraZeneca.
- Packer reports consulting fees/honoraria/speaking fees from Actavis, AstraZeneca, Boehringer Ingelheim, CSL Behring, Cytokinetics, Lilly, Moderna, Novartis, and Salamandra.
Related News


Comments