Plaque Type Equally Predictive of MI in Women and Men: SCOT-HEART
Low-attenuation plaque on CT predicts events in both sexes, so experts must seek other clues to improve women’s outcomes.

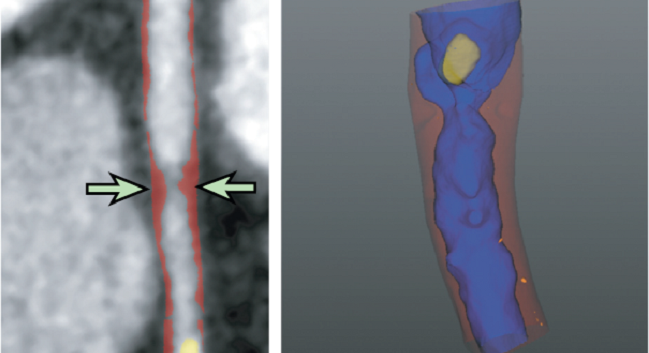
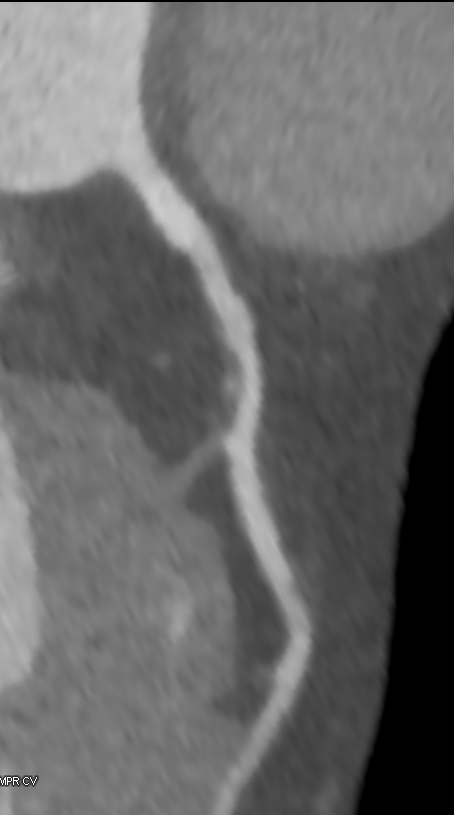
Quantitative plaque analysis, specifically the presence of low-attenuation plaque, is a robust predictor of cardiac endpoints in patients presenting with stable chest pain, no matter their sex, according to a new analysis of the SCOT-HEART trial.
A previous SCOT-HEART subanalysis confirmed the broad connection between low-attenuation plaque volume on CT and MI risk and strengthened the argument for using this imaging modality above other traditional risk scores and markers. The current findings, published online this week ahead of print in JACC: Cardiovascular Imaging, show sex has no effect on this association.
“For women who come to the hospital with stable chest pain, we know that there are differences—they are less likely to have atherosclerotic plaque of all the types compared to men,” lead author Michelle C. Williams, MBChB, PhD (University of Edinburgh, Scotland), told TCTMD. “But when they have their heart attacks—women who actually come to the hospital with a heart attack—those women have the same types of plaque and the same patterns of plaque compared to the men.”
Simply put, she explained, “when women come to hospital with symptoms of a heart attack, we should be treating them the same as men. Often we underestimate, don't think that we need to investigate, but the answer is we should do just as much as in men.”
Commenting on the study for TCTMD, Juan Lopez-Mattei, MD (MD Anderson Cancer Center, Houston, TX), agreed, noting that he was not surprised to see a lack of sex effect. “It definitely brings to our attention that the presence of low-attenuation plaque has to be seriously considered in symptomatic patients. And these patients perhaps will need way more-aggressive preventive care to reduce adverse outcomes,” he said.
For Kavitha Chinnaiyan, MD (Beaumont Health System, Royal Oak, MI), these findings confirm the need to shift focus away from simply comparing men and women toward a “biological understanding” of how disease manifests in each of those two populations. “Again and again we have had women being compared to men, and I think we need to move beyond that a little bit and compare women that have disease and bad outcomes to other women who don’t,” she told TCTMD, citing the possible roles of hormones and cancer therapy in cardiovascular disease. “I don’t think we have a good handle on why some women are more prone to bad outcomes than others.”
Lowdown on Low-Attenuation Plaque
For the study, Williams and colleagues compared outcomes between 772 women and 997 men who underwent coronary CTA as part of the SCOT-HEART trial.
Compared with men, women were more likely to have normal coronary arteries; were less likely to have adverse plaque characteristics; and had lower total, calcified, noncalcified, and low-attenuation plaque burdens (P < 0.001 for all). Women were also less likely to have a quantitatively-assessed low-attenuation plaque burden > 4% (41% vs. 59%; P < 0.001).
The 1.4% of women who experienced MI over a median follow-up of 4.7 years had similar total, noncalcified, and low-attenuation plaque burdens as the 3% of men who had MI. However, the men had higher calcified plaque burden.
On multivariate analysis, low-attenuation plaque burden independently predicted fatal or nonfatal MI (HR 1.71; 95% CI 1.22-2.39) regardless of sex, visually assessed obstructive disease, and cardiovascular risk score.
The biggest hurdle to including quantitative assessment of the atherosclerotic plaque in clinical practice right now is time, according to Williams. “The next thing we need is some more automation in the assessment of these CT scans [with] machine learning or [artificial intelligence] that will help us get these numbers into the scans much quicker and much more easily,” she said. “At the moment, there's extra information on these CT scans which is currently locked away and we never know about. Quantification can give us this information, but we just need it to be a bit quicker so that we can use it in clinical practice.”
Personalized Medicine
At this point, “there’s enough data from my standpoint on why cardiac CT is so relevant in stable patients with symptoms” that the focus now needs to shift to implementation, Lopez-Mattei said. “What are we going to do with all this rich data of coronary CT being so robust in prognostication?”
Chinnaiyan added that imagers have the responsibility to take all the data provided by CT and illustrate why certain plaques may be more problematic than others and lead to adverse events. “This plaque characterization has huge implications with regard to even what we want to do with patients,” she said. “How much more aggressive will we be with preventive efforts and perhaps even have a lower threshold for additional invasive testing if need be if patients are symptomatic whether the patient is male or female?”
I don’t think we have a good handle on why some women are more prone to bad outcomes than others. Kavitha Chinnaiyan
The true potential of CT is that it can be used to personalize care, Lopez-Mattei said. “Two patients with nonobstructive coronary artery disease are not the same—they might have different plaque composition and perhaps different outcomes,” he said. “Perhaps in the future coronary CT may be used to personalize medicine even more and tailor certain treatments.”
Future research should focus on more-specific patient subgroups, like the effects of radiation therapy on plaque characteristics, he continued. “There are other groups of patients that will benefit as well from studying plaque characterization for prognostication , but I think we have pretty good data showing the prognostic strength of coronary CT. This just strengthens it even more.”
Next up, Williams said the SCOT-HEART 2 trial will give more information as to if CT can add any benefit to risk assessment and outcome improvement in asymptomatic patients. “Atherosclerotic plaque will be part of that,” she said. “We now know what CT shows us in patients who have stable chest pain, but the next question is what about asymptomatic people. Can we improve outcomes for them as well? And do these sex differences and similarities persist?”

Yael L. Maxwell is Senior Medical Journalist for TCTMD and Section Editor of TCTMD's Fellows Forum. She served as the inaugural…
Read Full BioSources
Williams MC, Kwiecinski J, Doris M, et al. Sex-specific computed tomography coronary plaque characterization and risk of myocardial infarction. J Am Coll Cardiol Img. 2021;Epub ahead of print.
Disclosures
- Williams reports receiving support from the British Heart Foundation and the Chief Scientist Office of the Scottish Government Health
- Lopez-Mattei reports no relevant conflicts of interest.
- Chinnaiyan reports an institutional research grant from HeartFlow and serves as an unpaid clinical mentor for HeartFlow.
Related News



Comments