Pre-TAVI PCI Linked to More Late Bleeding, With Implications for Survival
The findings should remind operators to consider whether PCI is absolutely needed, and to take care with antithrombotic choices,


Approximately one in 10 patients who undergo PCI as part of pre-TAVI workup have late major bleeding events that increase their risk for death and disability, according to a multicenter study of patients from Canada, Europe, and Brazil.
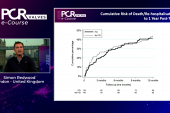
At 4 years, 43.9% of patients with late bleeding events had died versus 36% of those without bleeding events (P = 0.034), with late bleeding identified as an independent predictor of all-cause mortality after TAVI.
“One of the important factors that was associated with an increased risk of bleeding events was the combination of different drugs, particularly in those patients requiring anticoagulation,” senior study author Josep Rodés-Cabau, MD, PhD (Laval University/Quebec Heart & Lung Institute, Canada), told TCTMD. This suggests a need to focus efforts on decreasing the period of time where combination drug therapy is needed or avoiding PCI altogether, if possible, he added.
The findings may add additional caution on the backdrop of the ACTIVATION trial results, which found that PCI before TAVI in patients with at least one significant coronary stenosis did not improve survival or hospital-free survival over the next 12 months. In that study, PCI patients had a tendency toward increased bleeding that was primarily driven by the increased use of dual antiplatelet therapy (DAPT).
“Our study shows that bleeding events are frequent in this population, and not only in [terms of] periprocedural bleeding, which is what we have seen much of the focus on at this point,” Rodés-Cabau said. “They can and do occur later on . . . and can potentially be prevented by adjusting the antithrombotic treatment in this elderly and fragile population.”
In an accompanying editorial, Paolo Calabrò, MD, PhD (University of Campania Luigi Vanvitelli, Caserta, Italy), and Felice Gragnano, MD, PhD (Sant’Anna and San Sebastiano Hospital, Caserta, Italy), point out that although no RCT has sought to identify the optimal antithrombotic regimen in patients needing PCI and TAVI, decisions regarding dual or triple antithrombotic regimens should be based on coronary risk.
“Short DAPT of 1 to 3 months followed by P2Y12 inhibitor monotherapy has shown a favorable balance between ischemic protection and bleeding after PCI, regardless of procedure complexity,” they write “This strategy may be an attractive choice when PCI is performed in TAVR candidates and would allow DAPT discontinuation before or shortly after TAVR in most cases.”
Another option is P2Y12 inhibitor monotherapy in place of aspirin to reduce CV events as well as GI and intracranial bleeding, Calabrò and Gragnano say.
In the study, published this week in JACC: Cardiovascular Interventions, approximately 46% of all late bleeding events were GI in nature, with intracranial bleeds accounting for about 16%.
“If chronic oral anticoagulation is required, triple therapy should be stopped within 1 week after PCI; dual therapy should be continued for 6 months (shortened to 1-3 months if concern about bleeding prevails), followed by anticoagulation alone,” Calabrò and Gragnano add. “Additional transcatheter intervention with left atrial appendage occlusion in atrial fibrillation patients may be an option to withdraw anticoagulation, but we need evidence.”
That evidence may well come from the ongoing WATCH-TAVR trial, Rodés-Cabau noted. Initial data from that trial are set to be presented at the upcoming TCT meeting in October.
Nearly 30% of Bleeds Life-threatening
Led by Marisa Avvedimento, MD (Laval University), the researchers enrolled 1,457 consecutive patients (mean age 82 years; 41.5% women) who underwent a PCI within 3 months of TAVI and were alive at 30 days after TAVI. The median time between PCI and TAVR was 31 days. By 4 years, 116 patients (7.9%) had experienced late bleeding events, which were defined according to the Valve Academic Research Consortium-2 criteria and occurred more than 30 days after TAVI.
More than 50% of all late bleeding was classified as being major and 27.6% was life-threatening or disabling, occurring at a median of 10.2 months and 6.3 months, respectively, after the TAVI procedure.
In multivariable analysis, periprocedural major bleeding and the combination of antiplatelet and anticoagulation therapy at discharge were independently associated with an increased risk of late bleeding. An additional analysis found that DAPT was a common denominator among those with major and life-threatening bleeding, while oral anticoagulation was the most frequent regimen in those with minor bleeding.
At a median follow-up of 15 months after the late bleeding event, 56% of patients had died. Compared with patients who did not have late bleeding, those who did had higher rates of CV death (11.2% vs 8.7%; P = 0.010), ACS (16.4% vs 7.5%; P < 0.001), major stroke (15.5% vs 5.2%; P < 0.001), CV rehospitalization (50.9% vs 23.3%; P < 0.001), and major adverse CV and cerebrovascular events (59.5% vs 31.1%; P < 0.001). Late bleeding events were a key, independent predictor of all-cause mortality after TAVI (HR 1.39; 95% CI 1.05-1.83).
When Less Is More
“For the first time we saw that patients that had an episode of bleeding periprocedurally or in the days following the TAVI procedure were at higher risk of late bleeding events, meaning that it seems that when you bleed once, your likelihood of having more bleeding episodes increases,” Rodés-Cabau told TCTMD.
According to Calabrò and Gragnano, the potentially actionable message here is that removing the source or predisposing factors for early bleeding may help to prevent late events.
“These findings underscore the need for improved estimation of coronary, cerebrovascular, and bleeding risk to advance the existing process of care, particularly in light of the increasing demand for TAVR in lower-risk patients (the wider the risk spectrum, the more important individualized therapeutic approaches become),” they write.
Rodés-Cabau said given the dearth of solid data in this area, he would hope that heart teams take the findings into consideration when evaluating CAD in the pre-TAVI workup and avoid PCI whenever possible in patients with stable CAD.
“I think that that when you are evaluating whether or not to perform PCI in these patients, these increases in bleeding risk should be taken into account [because] when you are performing the PCI, you are already committed,” Rodés-Cabau said. “There are studies ongoing now trying to evaluate the potential advantages of PCI in these patients, but these trials will take several years to get the primary results. The data from our study goes in the same direction as what we see in the coronary field, which is that the concept of ‘less is more’ perhaps is becoming more accepted.”

L.A. McKeown is a Senior Medical Journalist for TCTMD, the Section Editor of CV Team Forum, and Senior Medical…
Read Full BioSources
Avvedimento M, Campelo-Parada F, Munoz-Garcia E, et al. Late bleeding events in patients undergoing percutaneous coronary intervention in the workup pre-TAVR. J Am Coll Cardiol Intv. 2023;16:2153-2164.
Calabrò P, Gragnano F. Bleeding in patients undergoing PCI and TAVR: combining coronary and valve procedures raises new challenges. J Am Coll Cardiol Intv. 2023;16:2165-2168.
Disclosures
- Rodés-Cabau has received institutional research grants and speaker/consultant fees from Edwards Lifesciences and Medtronic.
- Avvedimento, Calabrò, and Gragnano report no relevant conflicts of interest.
Related News

Comments