Preventing TAVR Obstruction of Coronary Arteries Remains a Challenge
Attempts to align TAVR and native commissures were modestly successful with self-expanding valves, but not with Sapien 3.

Attempts to improve commissural alignment during TAVR with commercially available transcatheter heart valves, a technique that would later facilitate access to the coronary arteries, yield mixed results, according to the results of a new study.
Investigators led by Gilbert Tang, MD (Mount Sinai Health System, New York, NY), say that controlling the initial deployment of Sapien 3 (Edwards Lifesciences) by crimping the valve at specific orientations to the delivery catheter had no impact on commissural alignment or coronary overlap. They had better success with the CoreValve Evolut (Medtronic) and Acurate Neo (Boston Scientific) transcatheter valves, but even there the results weren’t ideal.
“Despite our best efforts, we weren’t able to get consistent commissural alignment,” Tang told TCTMD. “It was essentially random for the balloon-expandable valve and better for the self-expanding valves.”
The study, which was published online before print March 16, 2020, in JACC: Cardiovascular Interventions, highlights a growing concern among operators implanting transcatheter heart valves in younger, lower-risk patients, and dashes some of the earlier optimism from a pilot study showing that aligning currently available TAVR devices at the time of the procedure could mitigate risks down the road. With the focus now on “lifetime management,” Tang said they have to think about future procedures, such as PCI, or possibly a second TAVR if, or when, the first valve fails.
“In TAVR initially, they were elderly patients who rarely needed a diagnostic cath or PCI,” he said. “Also, it was rare where the valve failed and the patient required a second TAVR procedure. Now, in 2020, it’s different ball game. Essentially anybody in the United States can undergo TAVR if they have symptomatic severe aortic stenosis and their anatomy is suitable. A lot of these patients are younger—they’re in the 70s and some are in their 60s—so the likelihood of them needing an angiogram or PCI is going to be higher than in a much older patient. We also know that the longevity of these valves is not forever. At some point, these valves will fail, just like surgical valves.”
In surgery, he explained, the native aortic valve leaflets are removed when the new valve is implanted and the surgical valve is aligned with the native commissures to prevent coronary obstruction. With TAVR, the native leaflets are not resected while the new transcatheter heart valve is placed within it, but there has been no way to predictably align the commissures with the native valve.
Some Improvement, but It’s Not Perfect
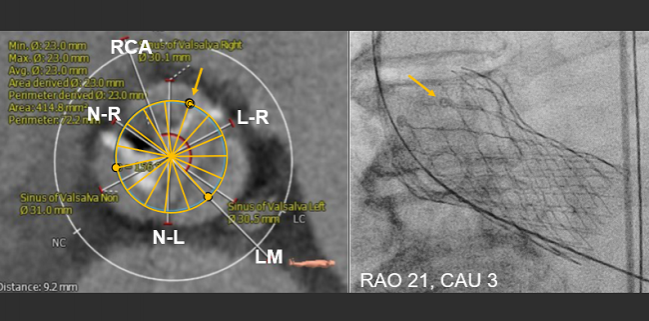
In the new study, which included 828 patients undergoing TAVR at 5 centers, investigators wanted to determine if they could intentionally rotate the delivery catheter, or crimp or prepare the valve with a specific orientation, to achieve better commissure alignment. As in previous studies, the group recorded aortograms and the final position of the Sapien 3, Evolut, and Acurate Neo valves during the procedure. Using various markers on the different valves, such as the C-tab on Evolut, for example, they co-registered the orientation of the valve to the pre-TAVR CT image.
To track the initial deployment orientation of Sapien 3, they crimped one commissure at 3, 6, 9, or 12 o’clock (relative to the delivery catheter). The “hat” marker with Evolut and the commissural tab position of Acurate Neo during initial deployment were categorized as center back (CB), inner curve (IC), outer curve (OC), or center front (CF). These initial positions of the valve were then matched with the final valve orientation.
Regardless of how Sapien 3 was crimped initially, it had no impact on final commissural alignment, with 51.3% of patients having either one or both coronary arteries overlapping with one valve commissure. With Evolut, there was overlap with one or both coronary arteries in 31.0% of cases, but the extent of coronary overlap was significantly reduced when the hat marker was positioned OC/CF during initial deployment. With Acurate Neo, 51.0% of patients had the valve commissure overlap with one or both coronary arteries, but the study suggested that orienting the commissural tab position to CB or IC improved coronary access.
To TCTMD, Tang said the frame height of Sapien 3 is shorter than the other supra-annular valves, which makes coronary access a little easier. However, it might still pose a problem for redo TAVR if the first device has leaflets extending close to or above the sinotubular junction, which would occlude the coronary arteries if a second device is implanted. Evolut, a supra-annular, self-expanding valve, is a taller device and its height can cause potential problems for physicians looking to gain coronary access, he said, but the hat marker can be tracked and this does improve commissural alignment.
“It’s not perfect, but these devices are not designed for commissural alignment so 100% perfect is not expected,” said Tang, referring to Evolut.
With Acurate Neo, which is available in Europe but not in the US, he noted that coronary access might also be an issue even though the valve has a low frame profile, especially if the tall commissural posts faces a coronary orifice. Like the other valves, redo TAVR could be complicated by the leaflets extending up to or above the sinotubular junction.
‘Call to Arms’
The new findings are a “call to arms,” said Tang, telling TCTMD that the field needs manufacturers to design valves and delivery systems that can achieve commissural alignment. Data from the Low-Risk Trial led by Ron Waksman, MD (MedStar Washington Hospital Center, DC), suggest that commissural alignment with the Sapien 3 valve could also not be achieved, he added. The newer-generation valves, such as JenaValve (JenaValve Technology) and J-Valve (JC Medical), are designed to align with the native valve commissures for deployment but are not currently available in the US.
“Right now, with certain valves we can try to improve alignment, and it’s not always successful, but based on the current technology, operators should still try to make it happen,” he said.
In an editorial, Hasan Jilaihawi, MD (NYU Langone Medical Center, New York, NY), praises the researchers for their efforts highlighting the issue and their technical attempts to overcome it. He points out, though, that while they were able to make technical modifications to “modestly” improve commissural alignment with Evolut, “it is unlikely to change the fact that coronary reaccess remains considerably easier with Sapien 3 than CoreValve, a limitation with uncertain future impact to patients with coexisting coronary artery disease.”
With repeat TAVR procedures, commissural misalignment that can occur with both Evolut and Sapien 3 can cause a “cylinder effect,” he says. This is a phenomenon that occurs when coronary perfusion is limited by the leaflets of the first device creating a “seal” once a second valve is implanted. Safety and efficacy of the Basilica procedure—which involves intentionally lacerating the bioprosthetic or native leaflet to prevent coronary artery obstruction—has not yet been demonstrated for repeat TAVR, states Jilaihawi.
Like Tang, he calls on device manufacturers to develop new valves, or new systems, that help operators align the commissures to keep future procedures, such as PCI, viable options for patients.
Photo Credit: Gilbert Tang

Michael O’Riordan is the Managing Editor for TCTMD. He completed his undergraduate degrees at Queen’s University in Kingston, ON, and…
Read Full BioSources
Tang GHL, Zaid S, Fuchs A, et al. Alignment of transcatheter aortic-valve neo-commissures (ALIGN TAVR): impact of final valve orientation and coronary overlap. J Am Coll Cardiol Intv. 2020;Epub ahead of print.
Jilaihawi H. When the (commissural) stars (mis)ALIGN. J Am Coll Cardiol Intv. 2020;Epub ahead of print.
Disclosures
- Tang reports serving as a physician proctor for Edwards Lifesciences and Medtronic as well as consulting for Medtronic.
- Jilaihawi reports consulting for Edwards Lifesciences, Boston Scientific, Medtronic, and Venus Medtech. He reports grant/research support from Medtronic and Abbott Vascular.
Comments