Shockwave Lithotripsy May Ease Transvenous Lead Extraction
It feels “like we’re taking out leads that are 1 year old even if they’re 20 years old,” a researcher says. An RCT is being planned.

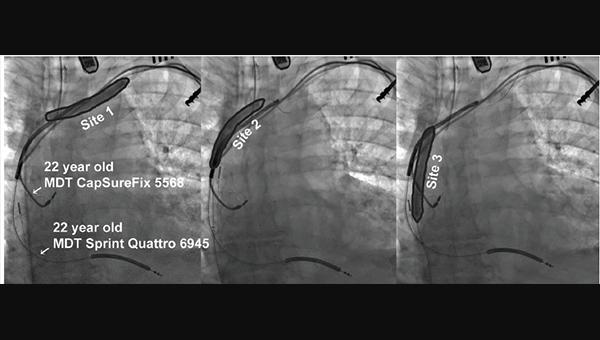
Typical balloon placement and pretreatment sites relative to pacing/defibrillation leads. Photo Credit: J Am Coll Cardiol EP. Central Illustration (adapted).
{kind=link}
Pacemaker and defibrillator leads encased in dense calcifications may be easier to remove after pretreatment with the Shockwave intravascular lithotripsy system (Shockwave Medical), preliminary results from a single center suggest.
With an initial time investment of about 15 minutes, the approach saved an average of 26 minutes during active lead extraction compared with conventional removal techniques, Christopher Latanich, MD, and John Anderson, DO (both from the Heart and Vascular Institute, Essentia Health, Duluth, MN), reported recently in JACC: Clinical Electrophysiology.
Dense calcifications are commonly found on leads that have been in the body for many years and they make extraction both more challenging and riskier; they’re typically addressed with mechanical cutting tools over laser sheaths. But now, some physicians are exploring the use of the Shockwave system, which uses focused sonic pressure waves to break up calcified tissue. The technology was developed to treat kidney stones and has been evaluated in recent years for the treatment of peripheral and coronary artery disease.
Latanich told TCTMD that this initial experience in the setting of lead extraction suggests the potential for a “dramatic” reduction in time spent actively removing leads and “profoundly less” variability in the procedure, although he acknowledged the preliminary nature of the findings.
Before starting to use intravascular lithotripsy, it could take up to 6 hours to get all of the leads out during an extraction procedure, he said. The longest it’s taken after pretreatment with the Shockwave system has been about 50 minutes.
When areas of calcification are reached with cutting tools or laser sheaths after pretreatment, “it kind of feels like instead of hitting an actual rock, it feels like you get into some sand, so you can feel where it is but it goes through it really easily now,” Latanich said. “It’s been a huge change.”
It kind of feels like instead of hitting an actual rock, it feels like you get into some sand. Christopher Latanich
The study included 65 patients who underwent lead extraction at Essentia Health between October 2019 and April 2023 (after exclusion of patients whose leads were freely mobile and could be removed without extraction tools). Of those, 14 patients (with 30 leads) had pretreatment with the Shockwave intravascular lithotripsy system; the remaining 51 patients (with 126 leads) underwent conventional extraction.
Patient and procedural characteristics were similar in conventional and lithotripsy groups, with no significant differences in median patient age (67 vs 70), proportion of women (26% vs 21%), and median lead dwell time (10.8 vs 11.1 years). The median number of leads attempted for extraction was two in each group.
The average time spent actively extracting leads—defined as the time from when all device leads were prepared and the first cutting tool was advanced over the first targeted lead to the time when the last targeted lead was removed—was significantly shorter after Shockwave pretreatment. Median extraction time was 15 minutes after pretreatment and 28 minutes with conventional removal (P = 0.007). There was also significantly less variability in the time required for extraction after use of intravascular lithotripsy (P = 0.022).
Although there was no significant difference in the median number of tools required for extraction (2.0 in the conventional group and 1.5 in the Shockwave group; P = 0.284), “most later procedures were completed with a single cutting tool, whereas earlier procedures were typically performed using a series of cutting tools to assist lead mobilization,” Latanich and Anderson report.
Rates of procedural and clinical success didn’t differ between groups.
In terms of safety, there were two major complications during conventional extraction (a vascular laceration and a pericardial effusion requiring intervention) and one after pretreatment with the Shockwave system (a vascular laceration).
Additional studies, including a planned prospective randomized controlled trial, are needed to further explore the safety of pretreatment with lithotripsy, Latanich indicated. It’s unknown whether the technique can be used in the presence of tight strictures or severe stenoses, whether lithotripsy is increasing embolization of debris, and whether the pressure waves affect the electrical performance of leads that remain in the body, he said. “We have yet to see any sign of any long-term lead damage or abnormalities, but that’s definitely a question going forward.”
Moreover, it’s unclear what the cost implications may be. A mechanical cutting tool costs between $3,000 and $4,000, with the Shockwave system coming in at about $3,500, Latanich said. So essentially, he said, if use of intravascular lithotripsy eliminates the need for even one cutting tool, it will pay for itself. “The cost savings are potentially quite substantial, but we are quite a ways from being able to prove that.”
These questions need to be answered before making any recommendations for widespread use of this technique, Latanich indicated. But “when we do these, it now makes our extractions feel like we’re taking out leads that are 1 year old even if they’re 20 years old,” he added. “I find it very encouraging.”

Todd Neale is the Associate News Editor for TCTMD and a Senior Medical Journalist. He got his start in journalism at …
Read Full BioSources
Latanich CA, Anderson JA. Shockwave intravascular lithotripsy facilitated transvenous lead extraction. J Am Coll Cardiol EP. 2023;Epub ahead of print.
Disclosures
- Latanich reports having performed consulting and research work with Boston Scientific and Medtronic and being in the process of setting up a prospective randomized clinical trial with Shockwave to more exhaustively evaluate this technique, although he has not received any compensation for this work.
- Anderson reports no relevant conflicts of interest.
Related News



Comments