Should Moderate FMR Be Treated With M-TEER? Experts Duke It Out
There was a consensus that more data are needed to answer this question, with discussions about what such a trial would look like.


BOSTON, MA—Is the existing evidence strong enough to perform transcatheter edge-to-edge repair (TEER) in patients with heart failure (HF) and moderate functional mitral regurgitation (FMR)?
That question was put to two experts this week at THT 2026, with Stefan Anker, MD, PhD (Charité Universitätsmedizin Berlin, Germany), chair of the RESHAPE-HF2 executive committee, arguing that it would be appropriate to use M-TEER in this population today, though it’s not necessarily a must.
“When you do correct FMR using M-TEER, you have very good results,” Anker said. “There is no question that we should also treat patients with moderate FMR.”
Anker noted that guidelines indicate that MR should be treated, pointing to European HF guidelines with a class IIa recommendation to consider TEER in carefully selected patients with FMR who remain symptomatic despite optimal medical therapy, with no mention of severity. In addition, iCARDIO Alliance global implementation guidelines on HF strongly recommend performing M-TEER in patients with FMR graded 4+ (severe), with the intervention receiving a somewhat weaker “suggested” recommendation for those with 3+ (moderate) MR.
Though saying that “we need to treat” moderate FMR, Anker acknowledged also that “we need more data on it.”
Gregg Stone, MD (Icahn School of Medicine at Mount Sinai, New York, NY), a co-principal investigator of COAPT, took the more conservative approach, arguing “that we need randomized trials before you should be performing TEER in moderate MR and heart failure.”
Stone highlighted the results of COAPT, in which M-TEER had a “marked positive effect” in patients with severe MR and HF. There is, however, much residual risk, with nearly half of patients treated with M-TEER dying or being hospitalized for HF through 2 years of follow-up.
This indicates that “maybe we should be treating earlier, perhaps moderate FMR,” Stone said. “That’s a great hypothesis,” but randomized data just aren’t there yet to support it, he said.
M-TEER Can Be Considered
Highlighting the need to consider treatment, Anker cited a cohort study showing that moderate MR is associated with an increased mortality risk compared with no/mild MR (HR 1.29; 95% CI 1.20-1.38), though the relationship between mortality and MR was stronger for patients with severe regurgitation (HR 1.82; 95% CI 1.64-2.02). The increased mortality risk in patients with moderate FMR was supported by a review in JACC, which also showed greater risks of HF hospitalization and heart transplant in this group.
Surgery has not been shown to improve long-term survival in patients with moderate ischemic MR, but M-TEER with MitraClip devices (Abbott), has been associated with lower 1-year rates of HF hospitalization in patients with either 2+ or 3+ FMR before the procedure in the EXPANDed studies, Anker said.
He pointed out, too, that RESHAPE-HF2 included patients with FMR 3+ (56%) and 4+ (44%) who were well treated on guideline-directed medical therapy (GDMT). Based on effective regurgitant orifice area (EROA), the trial enrolled the “mildest” group of FMR patients when compared with COAPT and MITRA-FR, he said.
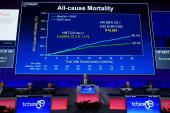
“And still, of course, you know that RESHAPE worked,” Anker told meeting attendees. Use of the MitraClip reduced rates of hospitalization for HF or CV death (primary composite endpoint) and HF hospitalization alone while improving quality of life. A subgroup analysis indicated no significant influence of either MR severity (P = 0.07 for interaction) or EROA (P = 0.45) on the primary endpoint.
He offered a compromise: “Basically, we can conclude that severe functional [regurgitation] is really something that you have to treat and less than severe—that definitely includes the moderates—can be considered for treatment. Yes, we may need more data, but we have quite a lot already.”
Not So Fast
Like Anker, Stone showed data demonstrating that moderate FMR was almost as prognostic as severe FMR in terms of long-term mortality risk in patients with chronic HF and pointed to the EXPANDed results showing comparable effects of M-TEER in patients with either moderate or severe FMR.
“So I’m making your case, Stefan,” Stone said. “However, all of this was unblinded data and . . . certainly for this analysis, there’s immortal time bias you have to take into account.”
There is other evidence to consider, too, Stone said. In COAPT, an analysis looking at residual MR 30 days after the procedure showed that patients who had moderate regurgitation had outcomes similar to those in patients with mild or less MR.
“[I’m] not sure that treating that would do anything,” Stone said.
He then compared the patient cohorts of COAPT, MITRA-FR, and RESHAPE-HF2, noting that they appear relatively similar but with major differences in LV end-diastolic volumes and EROAs because of variations in US and European inclusion criteria.
“Specifically, the European criteria, while at the time were considered severe, allowed patients with mild and moderate FMR to be entered into the trials, according to at least the EROA criteria,” Stone said. “So while COAPT enrolled almost all severe FMR, the MITRA-FR trial had about 50% of patients who were not severe. And, in fact, in RESHAPE-HF2, about 50% of the patients were moderate and almost a quarter were mild FMR according to EROA criteria.”
In terms of outcomes, there was a “huge benefit” of M-TEER in COAPT, no significant benefit in MITRA-FR, and an intermediate benefit in RESHAPE-HF2, Stone said. Regarding RESHAPE-HF2, although there was not a significant interaction between MR severity and outcomes, the group that “clearly benefited” from treatment was the patients with severe FMR, with no significant benefits in those with moderate or mild FMR, he said.
That suggests the need for additional data and “a dedicated study that really defines what moderate FMR is and a randomized trial before TEER is widely recommended” in that group, Stone said.
Though the latest European HF guidelines don’t mention MR severity in their M-TEER recommendations for FMR, the valvular heart disease guidelines released last year are more explicit, providing class I and IIb recommendations for severe symptomatic FMR and none for moderate FMR, Stone highlighted.
“So let’s have a randomized trial. Let’s see if this really works,” he said. “And hopefully pretty soon we’ll be able to make such an announcement.”
Mulling a Trial in Moderate FMR
A panel discussion following the debate tackled what a trial of M-TEER in moderate FMR would look like, with questions around the criteria that should be used to select participants and the potential impact of improved GDMT, including greater use of angiotensin receptor-neprilysin inhibitors and sodium-glucose cotransporter 2 inhibitors, since COAPT, MITRA-FR, and RESHAPE-HF2 were conducted.
“I’m a little bit afraid that these kinds of trials become more and more difficult to enroll patients, because our heart failure docs will insist on putting patients on . . . the golden four [pillars of GDMT],” Nicolas Van Mieghem, MD, PhD (Erasmus University Medical Center, Rotterdam, the Netherlands), said. “How many of those patients will remain symptomatic with their moderate MR?”
Stone said that some patients will become asymptomatic with better medical therapy, “but I don’t think it’s going to be half the patients or 75% of the patients. When you look at the effect of any one of the drugs, they’re relatively modest.” For patients who are refractory to GDMT and continue to have symptoms and exercise limitations, he added, “I think it’s going to be great to test them. My hypothesis is that it will be effective with the right kind of trial.”
Beyond establishing the appropriate criteria to select patients with moderate FMR, it will also be important to avoid crossovers in any future trial, Stone said. “There’s no indication to treat moderate FMR right now. . . . And if the patient remains symptomatic in the control arm, and unless they develop severe FMR, we’ve got to make sure they don’t cross over.”
Linda Gillam, MD (Atlantic Health, Morristown, NJ), raised another issue to consider, noting that in practice, some patients who have apparently “maxed out” on GDMT can have therapy intensified after undergoing M-TEER. “I would hope that would be an outcome that you would capture,” she said.
Stone indicated that in COAPT, the investigators discouraged using better GDMT after the procedure to better isolate the effect of M-TEER. In a future trial in moderate FMR, however, “we are going to look at more of a strategy approach, and if the hemodynamics get better in the moderate FMR arm after treatment so you can further maximize GDMT, we’ll take advantage of that,” he said.

Todd Neale is the Associate News Editor for TCTMD and a Senior Medical Journalist. He got his start in journalism at …
Read Full BioSources
Multiple presentations. Presented at: THT 2026. March 2, 2026. Boston, MA.
Disclosures
- Anker reports grant/research support from Abbott Vascular and Vifor International; consulting fees/honoraria from Vectorious, AstraZeneca, Bayer AG, Boehringer Ingelheim, Brahms, Cardiac Dimensions, CVRx, Edwards Lifesciences, Impulse Dynamics, Novartis, Occlutech, V-Wave, Novo Nordisk, Scirent, Pulnovo, Berlin Heals, VisCardia, and Sensible Medical; and stocks/options from Cordio.
- Stone reports consulting for or having equity in Abbott, Valfix, Ancora, Cardiac Success, and HighLife, as well as receiving institutional grants from Abbott.
Related News


Comments