New ESC HF Guidelines Showcase SGLT2 Inhibitors, Tafamidis, Vericiguat, and COAPT
A guideline chair acknowledged the new document is already in need of an update—a “nice” problem to have, said Marco Metra.


Heart failure (HF) guidelines released at the European Society of Cardiology (ESC) Congress 2021 yesterday give a new class I recommendation for sodium-glucose cotransporter 2 (SGLT2) inhibitors in the setting of HF with reduced ejection fraction (HFrEF), and they urge physicians to initiate all four recommended drug categories—ACE inhibitors/angiotensin receptor-neprilysin inhibitors (ARNIs), beta-blockers, mineralocorticoid receptor antagonists (MRAs), and SGLT2 inhibitors—as swiftly and safely as possible.
“This is not only a name change, but this means that patients with an ejection fraction below 50% . . . have a milder form of heart failure with the reduced ejection fraction, and this means that likely the same drugs that are used in patients with reduced ejection fraction may also be started in the patients with an ejection fraction from 41% to 50% or even maybe a little bit more,” guideline co-chair Marco Metra, MD (University of Brescia, Italy), told TCTMD. “And this applies to all the drugs that are indicated for heart failure with reduced ejection fraction.”
But given the timing—the guidelines were released just hours ahead of the presentation of the EMPEROR-Preserved trial—the advice, for some, is already woefully out-of-date.
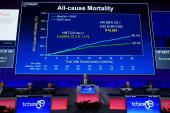
Widely hailed as a landmark trial, EMPEROR-Preserved marks the first major, positive trial in HFpEF with benefits also seen in “midrange” patients. The finding prompted some in the Hot Line session to speculate that the time had come to think less about ejection fraction cutoffs and more about global cardiac dysfunction, with everything above 60% defined as “normal.”
For now, however, the heart failure guidelines don’t include the latest empagliflozin (Jardiance; Boehringer Ingelheim/Eli Lilly) data. They specifically define a more mildly reduced EF group, and they explicitly state: “To date, no treatment has been shown to reduce mortality and morbidity in patients with HFpEF.”
Key Changes in the Guidelines
Walking TCTMD through some of the key changes in the 2021 heart failure guidelines, Metra highlighted the strengthened recommendations for SGLT2 inhibition in HFrEF. Both empagliflozin and dapagliflozin (Farxiga; AstraZeneca) now have a class I, level of evidence A indication for reducing HF hospitalizations and death.
That top tier is shared with ACE inhibitors, beta-blockers, and MRAs, with the ARNI sacubitril/valsartan (Entresto; Novartis) getting a class I, level of evidence B recommendation as a replacement for an ACE inhibitor to reduce the risk of HF hospitalization or death. “So the first major change to the guidelines is that we have four classes of drugs indicated for all patients with heart failure and reduced ejection fraction,” Metra said.
Roy Gardner, MBChB, MD (Golden Jubilee National Hospital, Glasgow, Scotland), who summarized part of the latest guidelines during a dedicated session Friday, further emphasized that the aim is to initiate all four medicine classes as swiftly and safely as possible. A new, simplified treatment algorithm for HFrEF is provided in the update.
A special section devoted to diabetes urges that all heart failure patients with type 2 diabetes should be treated with an SGLT2 inhibitor (class I, level of evidence A).
Vericiguat (Verquvo; Merck Sharp & Dohme) enters the guidelines, following the positive results from the VICTORIA trial. The soluble guanylate cyclase stimulator gets at IIb recommendation, meaning it “may be considered in patients in NYHA class II-IV who have had worsening HF despite treatment with an ACE inhibitors (or ARNI), a beta-blocker, and an MRA to reduce the risk of CV mortality or HF hospitalization.”
The recommendation for implantable cardioverter-defibrillators to reduce the risk of sudden death or all-cause mortality in patients with NYHA class II-III symptoms and nonischemic etiology is softened slightly, moving from class I in 2016 to class IIa in 2021. Cardiac resynchronization therapy for symptomatic patients with HF in sinus rhythm with a QRS duration of 130-149 ms, left bundle branch block QRS morphology, and an LVEF ≤ 35% despite best medical therapy gets a similar demotion.
Added Trial Evidence
Metra had other highlights, however. Special sections of the guidelines, he noted, tackle CV and noncardiovascular comorbidities including diabetes, hyperkalemia, cancer, atrial fibrillation (AF), and iron deficiency.
For this last, the guidelines incorporate AFFIRM-AHF, recommending that intravenous iron supplementation with ferric carboxymaltose “should be” considered in symptomatic HF patients recently hospitalized for HF and with LVEF < 50% and iron deficiency (class IIa). There is also a recommendation for all patients with HF to undergo periodic screening for anemia and iron deficiency (class Ia).
Patients with AF get special attention, too, with direct oral anticoagulants (DOACs) being given preference over vitamin K antagonists (moving from class IIa to class I); beta-blockers move down from class I to IIa. DOACs also get a class I, level of evidence A recommendation for all patients with AF, HF, and a CHA2DS2-VASc score ≥ 2 in men or ≥ 3 in women. Catheter ablation, however, moves up from class IIb to class IIa “in cases of a clear association between paroxysmal or persistent AF and worsening of HF symptoms, which persist despite medical therapy.”
Tafamidis (Vyndaqel; Pfizer), tested in ATTR-ACT, also makes its debut in the guidelines, getting a class I recommendation for both hereditary and wild-type transthyretin cardiac amyloidosis and cardiomyopathy in the setting of NYHA class I or II symptoms to reduce symptoms, CV hospitalization, and death.
On the structural heart disease front, the guideline writers recommended that patients with heart failure and severe aortic stenosis be treated with either SAVR or TAVI to reduce mortality and improve symptoms (class I, level of evidence B) and that the choice of intervention be made by the heart team, incorporating patient preference (class I, level of evidence C).
The COAPT and MITRA-FR trials get their due in this update, as well, something Metra characterized as a “major change” to the guidelines. Now, percutaneous edge-to-edge mitral valve repair is given a class IIa, level of evidence B recommendation, meaning that clip repair “should be considered in carefully selected patients with secondary mitral regurgitation, not eligible for surgery and not needing coronary revascularization, who are symptomatic despite optimal medical therapy (OMT) and who fulfill criteria for achieving reduction in HF hospitalizations.” A class IIb, level of evidence C recommendation is given for transcatheter edge-to-edge repair in “carefully selected patients with secondary mitral regurgitation, not eligible for surgery and not needing coronary revascularization,” who are “highly symptomatic despite OMT and who do not fulfill criteria for reducing HF hospitalization.” CABG and mitral valve surgery should be considered (class IIa, level of evidence C) in patients with HF, severe secondary mitral regurgitation, and CAD who require revascularization.
To TCTMD, Metra explained that the guidelines negotiated the disparate findings of MITRA-FR and COAPT by specifying that patients should meet the strict enrollment criteria stipulated by the COAPT trial, adding that the differences in exclusion criteria between the two trials, and particularly the decision to exclude patients with right ventricular dysfunction in COAPT, have now been widely accepted as a key reason for the differences between the two trial results.
Recommendations for home telemonitoring, both noninvasively and with implantable pulmonary artery sensors, are unchanged in the new guidelines, but may also be up for reconsideration in the future, some predicted yesterday. GUIDE-HF, presented in Friday’s ESC Hot Line session, missed its primary endpoint but hinted at benefits of pulmonary artery pressure management in less symptomatic HF patients.
Speaking to the conundrum of having practice guidelines that always seem to fall behind the latest evidence, Metra pointed out that this update has been in the works for years.
“The guideline committee had our first meeting . . . in July 2019, so it was a process taking 2 years, 31 task force members, and more than 70 or 80 reviewers. All the recommendations were voted on, and sometimes voted on again and again,” he said. “So, absolutely, we need more-frequent updates of the guidelines to include new findings, but in the end, it's a very good thing because this means that we have continuous improvement in the treatment of the patients with heart failure.”
Three years ago, he noted, many of the things now included in this update “seemed almost impossible,” most notably the kind of impact demonstrated by the SGLT2 inhibitor trials and COAPT.
“Things moving forward is a good thing,” he said. Guidelines need to be acknowledged as consensus documents that attempt to “crystalize” a fast-moving field.
Theresa McDonagh, MBChB, MD (King’s College London, England), one of the guideline chairs, made a similar point during the EMPEROR-Preserved session yesterday, noting that the cutoff for evidence to be considered for this update was the end of March 2021.
“Guidelines are updated rather slowly,” she conceded. “That doesn’t stop people starting to think about using [new evidence] now,” she said, adding that the EMPEROR-Preserved results still need to be considered by regulatory bodies. “Guidelines don’t have to drive things from top down. They’re not commandments. They can be bottom-up implementation as well.”

Shelley Wood was the Editor-in-Chief of TCTMD and the Editorial Director at the Cardiovascular Research Foundation (CRF) from October 2015…
Read Full BioSources
McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;Epub ahead of print.
Disclosures
- Guideline committee disclosures have been published online.
Related News


Comments