Soft Robotics Approach Brings Hemodynamics to 3D Aortic Models
The addition of patient-specific sleeves and pneumatics can “activate” 3D printed models to better plan for procedures.

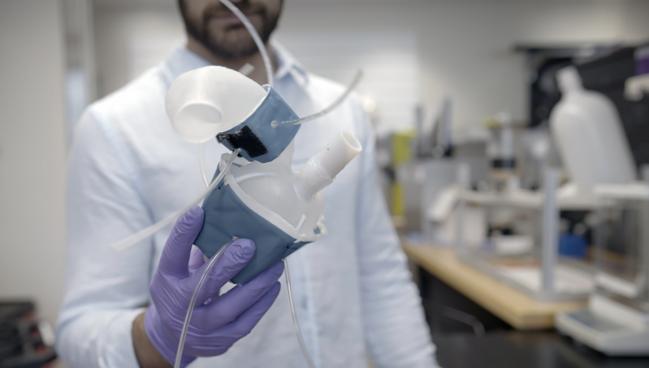
Photo Credit: Melanie Gonick (Massachusetts Institute of Technology)
New technology is allowing researchers to not only 3D print a replica of a patient’s heart, and specifically their aorta, but also use pneumatics to mimic individual hemodynamics.
For years, clinicians have been incorporating 3D models—both computerized and printed—based on CT data to plan procedures, especially in the structural heart space. Now researchers are taking things a step further by inventing a way to use patient-specific soft robotic sleeves to better mimic the effects of, in this case, aortic stenosis in a pumping heart.
This kind of modeling might not be needed for straightforward cases, but “there are definitely ‘edge’ cases, which are more challenging to make decisions on,” lead author Luca Rosalia, MEng (Health Sciences and Technology Program, Harvard–Massachusetts Institute of Technology, Cambridge, MA), told TCTMD. “We can recreate those anatomies, etiologies, and hemodynamic parameters for patients that might be more challenging to treat or make decisions on, [and] you are going to envision the system to be used for those patients.”
The newness of these models is related to the fact that they are active as opposed to rigid, senior author Ellen Roche, PhD (Massachusetts Institute of Technology), told TCTMD. “We have a biomimetic sleeve that can recreate the aortic profile and it can be dynamic,” she explained. “With the cardiac cycle, you can change the profile. And then similarly with the ventricle, we add the sleeve to make it active so we can have inherent pumping motion in the wall of the ventricle. We do not have to connect it to a piston pump or whatever to drive the flow around a flow loop. This printed model has a sleeve that generates that motion and the resulting hemodynamics itself.”
Their findings were published online recently in Science Robotics.
Manufacturing the Models
To derive their models, the researchers used clinical and imaging data from CT, transthoracic and/or transesophageal echocardiography, and LV catheterization for 15 patients (40% female; mean age 78 years) with aortic stenosis (AS). In total, four patients had bicuspid valve anatomy, six had severe AS, 14 showed some evidence of aortic regurgitation, eight displayed thickening of the LV wall, and four had an LVEF below 40%.
They used commercially available 3D printers to print anatomical models of the patients’ LVs and aortas using a soft elastomeric photopolymer resin and designed patient-specific soft robotic LV and aortic sleeves.
“The platform designed and developed in this work is ultimately intended for high-fidelity testing and evaluation of medical devices for AS, procedural planning, and outcome prediction, as well as product selection personalized to each patient’s anatomy, hemodynamics, and disease state,” the researchers write. “Hence, we demonstrated its potential utility by implanting a TAVR and conducted retrospective clinical validation in a subset of our study cohort.”
Specifically, their model recreated each patient’s hemodynamic parameters, including mean and maximum transaortic pressure gradients, peak aortic flow velocity, and stroke volume, with “high accuracy.”
Currently, these models take between 24 and 48 hours to produce, according to Rosalia and Roche, but they are working toward speeding up the process so that it can be more readily adopted in clinical practice.
For the time being, Roche added, “we are using it now in the lab, and it helps with a lot of testing and understanding of biomechanics and tweaking of different parameters and looking at sensitivity to different cardiac parameters.”
Manufacturing the robotic parts of the model is potentially more involved than the efforts required to print the kind of rigid 3D models some institutions might already be familiar with, Rosalia said, but he doesn’t see this as too big of a challenge for adoption. “We are already looking into using some machine-learning algorithms to make these digital geometries from the patient scans even faster,” he added.
Additionally, because the material costs are low, Roche said she doesn’t expect there to be a “huge added cost” of creating these patient-specific models beyond the initial infrastructure needed to acquire and set up the 3D printers.
Going forward, Rosalia said he would like to be able to broaden the capabilities of their system to address other pathologies, further personalizing this approach to procedure planning. “We envision these patients coming into the clinic and getting their imaging done, and then their hemodynamic assessment [so that] these systems could be built and run,” he said. “Different types of devices can be tested to understand which one would give the best outcome for these patients. And we hope that this can ultimately help clinicians make decisions for their interventions.”

Yael L. Maxwell is Senior Medical Journalist for TCTMD and Section Editor of TCTMD's Fellows Forum. She served as the inaugural…
Read Full BioSources
Rosalia L, Ozturk C, Goswami D, et al. Soft robotic patient-specific hydrodynamic model of aortic stenosis and ventricular remodeling. Sci Robot. 8, eade2184 (2023).
Disclosures
- This work was supported by the National Science Foundation, the NIH National Heart Lung Blood Institute, the MathWorks Engineering Research Fellowship, the Fulbright-Turkey Fellowship, the Lausanne University Improvement fund, the SICPA Foundation, the NIH, and the Sarnoff Cardiovascular Research Foundation.
- Roche reports serving on the board of directors for Affluent Medical and Helios Cardio and the board of advisors for Pumpinheart; serving as a consultant for Holistick Medical; and being a cofounder of Fada Medical and Spheric Bio.
- Rosalia reports no relevant conflicts of interest.
Related News

Comments