Tricuspid Repair During Mitral Valve Surgery Prevents TR Progression
While concomitant surgery reduced TR grade, it was not associated with a lower risk of death in long-term follow-up.


Patients with moderate tricuspid regurgitation (TR) undergoing surgery for mitral valve disease have a significant improvement in TR grade, according to the results of a new study.
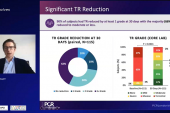
In early postoperative follow-up, more than 90% of patients with moderate TR who had concomitant tricuspid valve surgery had their TR grade reduced to mild or better, and researchers report this benefit was maintained long term.
Irsa Hasan, MD (Mayo Clinic, Rochester, MN), who presented the results of their retrospective series at the Society of Thoracic Surgeons (STS) annual meeting earlier this week, noted that while the current guidelines support the correction of severe TR during MV surgery, “the indication for tricuspid valve intervention for less-than-severe TR in the absence of right-heart failure or significant tricuspid annulus dilation is less clear.”
Tricuspid regurgitation is common in patients undergoing MV surgery for degenerative MR, and there are concerns that if mild or moderate TR is not fixed at the time of surgery, it might progress and result in adverse outcomes, such as an increased risk of death or worsening functional outcomes.
Just last week, the Cardiothoracic Surgical Trials Network (CSTN) published results from a randomized trial, presented last year at the American Heart Association meeting, showing that performing tricuspid annuloplasty in patients with mild-to-moderate TR at the time of MV surgery lowered the risk of progression to more severe TR. Follow-up in that study was just 2 years, however, and investigators, led by James Gammie, MD (Johns Hopkins School of Medicine, Baltimore, MD), say that long-term follow-up will be needed to determine the clinical benefit of reducing the TR grade.
In the Mayo Clinic series, however, the adjusted risk of death out to 12 years follow-up was not significantly different between those who underwent TR repair during MV surgery and those who did not. Additionally, the need for reoperation was similar between the two groups.
Focus on Moderate MR
The retrospective analysis included patients undergoing MV surgery with and without tricuspid surgery between 2001 and 2018. The researchers included patients with preoperative transthoracic (TTE) and at least one postoperative TTE (within 6 months), and they excluded patients with a previous MV or tricuspid valve procedure and those undergoing concomitant aortic-valve surgery.
In total, they identified 1,588 patients undergoing MV repair, of whom 25% had moderate TR and 7% had severe TR. Among the 404 patients with moderate TR—the focus of the analysis—103 patients had concomitant tricuspid valve surgery and 301 were left untreated. As noted, 40% of patients with moderate TR who underwent concomitant tricuspid valve surgery had their TR grade reduced to mild and 50% had only trivial or no TR at all in early postoperative TTE follow-up. Among those untreated, 6.6% had severe TR, 43.6% had moderate TR, and 34.6% had mild TR on postoperative TTE.
Regarding the long-term follow-up, those who had moderate TR treated during MV surgery “had generally a similar risk or probability of moderate or greater TR at 5, 10, and 15 years,” said Hasan. Compared with patients who didn’t have moderate TR treated during surgery, “the probability of worsening TR increased with time and these trends were generally similar for all of the preoperative [TR] grades,” she continued. The risk of uncorrected moderate or less TR progressing to severe TR was 5.4% at 5 years. Interestingly, the risk of progression to severe TR was not influenced by the size of tricuspid annulus diameter, but a diagnosis of preoperative congestive heart failure was associated with severe TR progression.
The rate of early pacemaker implantation was 3.0%, said Hasan. In the recent CSTN study, 14.1% of patients undergoing MV surgery with tricuspid annuloplasty required a new permanent pacemaker.
Rate of Pacemaker Implantation
Gorav Ailawadi, MD (University of Michigan, Ann Arbor), who moderated the STS session, questioned just how surgeons at the Mayo Clinic approach patients with moderate TR who require MV surgery given that their data showed there was no clinical impact of reducing TR grade, except that it prevented the progression to more severe TR.
“At this time, it’s still surgeon discretion,” said Hasan. “I don’t think there has been significant change just yet.” She noted that annulus diameter has been frequently used to guide decision making—with 4 cm typically being the cutoff to define tricuspid annulus dilation—but their results didn’t show that annulus diameter was predictive of progression to severe TR.
Session co-moderator Joanne Chikwe, MD (Cedars-Sinai Medical Center, Los Angeles, CA), focused on the rate of pacemaker implantation, noting that the low rate seen in the Mayo Clinic series is line with other studies. Ailawadi, who was one of the CSTN investigators, said the need for pacemaker implantation with tricuspid repair during MV surgery remains a “hot topic” due to the high rate observed in their study. The researchers are planning further analyses of the CSTN data to look for risk factors for conduction abnormalities requiring pacemakers.

Michael O’Riordan is the Managing Editor for TCTMD. He completed his undergraduate degrees at Queen’s University in Kingston, ON, and…
Read Full BioSources
Hasan I, Crestanello J, Daly R, et al. Impact of tricuspid regurgitation on late outcomes of mitral surgery. Presented at: STS 2022. January 31, 2022.
Disclosures
- Hasan reports no conflicts of interest.
- Ailawadi reports consulting for/serving on the advisory board/research or grant support from Abbott, Admedus, Atricure, CryoLife, Edwards Lifesciences, Medtronic, and W.L. Gore.
Related News

Comments