Ultralow-Temperature Cryoablation Promising for Monomorphic VT
The first-in-human results represent “an encouraging first step with a novel ablation source,” one expert says.

BERLIN, Germany—Treatment of monomorphic ventricular tachycardia (VT) with a novel ultralow-temperature cryoablation catheter (vCLAS; Adagio Medical) appears to be safe and effective in patients with either ischemic or nonischemic cardiomyopathy, according to the results of the first-in-human Cryocure-VT study.
There were no protocol-defined major adverse events related to the device or procedure, with good acute results in terms of eliminating VT, Atul Verma, MD (McGill University Health Centre, Montreal, Canada), reported earlier this week at the European Heart Rhythm Association Congress 2024.
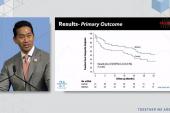
And by 6 months, 60.3% of patients remained free from any VT lasting more than 30 seconds and 81.0% remained free from implantable cardioverter-defibrillator (ICD) shocks.
These results, published simultaneously online in EP Europace, were in line with those from previous pivotal VT studies, Verma reported. “Further postmarket research is required and additional studies are in progress, including FULCRUM-VT, which will be the pivotal US trial,” he said.
Usha Tedrow, MD (Brigham and Women’s Hospital, Boston, MA), the discussant following Verma’s presentation, noted that there is a desire for better success rates with VT ablation; currently, the rates come in at around 60% with radiofrequency catheters. There are challenges in terms of mapping, with difficulty in identifying functional and intramural substrate, and in terms of ablation, with radiofrequency catheters having problems with fibrosis, calcification, chronic thrombus, and intramural scar, she said.
“We need a powerful but titratable energy source that we can use to reach into the deep intramural substrates without collateral damage,” said Tedrow.
Exploring whether the cryoablation system studied here is the answer, she pointed out that although the 60% rate of VT recurrence falls in line with prior studies, VT burden was reduced “very significantly.”
Safety and efficacy were “reasonable,” she said, adding that “it would be really interesting to see the results with more substrate guidance by imaging assistance that might help enhance the success rates.”
Overall, Tedrow concluded, “this is an encouraging first step with a novel ablation source.”
Cryocure-VT Study
VT ablation continues to be a “vexing problem” when using radiofrequency energy, Verma said, pointing to attenuated lesion depth in scar tissue, limited lesion depth even in normal tissue, and a persistent rate of complications in patients with cardiomyopathy.
A change in energy source for ablation may help improve the situation, he said. Ultralow-temperature cryoablation, which received CE Mark approval in Europe for the treatment of VT last month and remains investigational in the US, differs from traditional cryoablation in that it employs supercritical fluid nitrogen that prevents vapor lock and enables delivery through smaller-lumen catheters.
“So that’s really the key solution,” Verma said, adding that this type of ablation can penetrate both scar and normal tissue, with the depth of the lesion dependent on the length of the freeze.
Conducted at nine centers, Cryocure-VT was a first-in-human trial of this system in 64 adult patients (mean age 67 years; 95.3% men) with ischemic or nonischemic cardiomyopathy who were eligible for catheter ablation due to recurrent symptomatic sustained monomorphic VT. All patients were refractory to at least one antiarrhythmic drug and received an ICD prior to discharge.
Patients had a mean LVEF of 35%. Most (79%) had ischemic cardiomyopathy, with the remaining having nonischemic substrates.
For the procedure, intracardiac echocardiography was used in 68.8% of cases. The mean procedure time was 188 minutes, “which for a scar-based cardiomyopathy VT ablation procedure is quite reasonable,” Verma said. The mean number of lesions per patient was 8.9, with an average freeze time of 3.8 minutes per lesion.
Acute results were “really good,” Verma reported. The rate of primary success (no inducible clinical VT) was 94.4%, and the rate of secondary success (no inducible VT of any kind) was 85.2%. More than 97% of clinical VTs were eliminated.
The 6-month results in terms of freedom from recurrent sustained monomorphic VT or appropriate ICD therapy were similar regardless of the type of underlying cardiomyopathy. Among the patients who had had an ICD for at least 6 months prior to ablation, VT burden was reduced from a median of 4 ICD events to 0.
In terms of safety, there were no device- or procedure-related major adverse events within 30 days of ablation, although there were four serious adverse events—two trivial/small pericardial effusions (3.1%), one asymptomatic false aneurysm in 2-mm tissue (1.6%), and one case of hemodynamic instability during the procedure that required extracorporeal membrane oxygenation support (1.6%). All resolved without clinical sequelae.
More Research Needed
Commenting on the results for TCTMD, K.R. Julian Chun, MD (CardioAngiologisches Centrum Bethanien, Frankfurt, Germany), noted that “we are lacking lesion depth for VT ablation, and here comes a catheter which allows us to create very deep lesions. And it’s dose-dependent on the duration of the freeze, so therefore it may be an interesting device to really get deep lesions.”
This technology could be particularly useful for treating specific types of premature ventricular complexes, such as those in papillary muscle, because of the increased stability of the catheter when it adheres to the tissue, Chun said.
He said that his team will perform some cases with the system soon but added that these data are very preliminary. “We need to learn more,” he said. “We need to see how this works within a 3D mapping system . . . because of course we need to understand where to ablate, where is the substrate.”
Tedrow said, too, that even though safety was reasonable in this study, the occurrence of an asymptomatic false aneurysm in very thin tissue was potentially concerning. “We don’t know if we did routine imaging of all the patients if something . . . like that would be identified in more of the patients.”
More information also is needed, she indicated, into the mechanisms of the observed VT recurrences.

Todd Neale is the Associate News Editor for TCTMD and a Senior Medical Journalist. He got his start in journalism at …
Read Full BioSources
Verma A, Essebag V, Neuzil P, et al. Cryocure-VT: the safety and effectiveness of ultra-low-temperature cryoablation of monomorphic ventricular tachycardia in patients with ischaemic and non-ischaemic cardiomyopathies. Europace. 2024;Epub ahead of print.
Disclosures
- The trial was funded by Adagio Medical.
- Verma reports being a consultant for Biosense Webster, Medtronic, Adagio Medical, Medlumics, and Abbott.
Related News


Comments