When Early Cardiogenic Shock Isn’t Dealt With, Outcomes Can Suffer
Approximately one in four patients died, deteriorated to a higher shock stage, or were transferred for a higher level of care.


WASHINGTON, DC—Early-stage cardiogenic shock leads to poor outcomes but is underrecognized, with only one in four affected patients having any indication in their electronic medical record (EMR) that they even have it, according to a multicenter study presented here last week at the Society for Cardiovascular Angiography and Interventions (SCAI) 2025 Scientific Sessions.
SCAI SHOCK classifies the condition as: A (At risk), B (Beginning), C (Classic), D (Deteriorating), and E (Extremis). The current study of 500 patients focuses on those with stage B (defined as isolated hypotension or hypoperfusion).
One in four patients at this degree of shock severity ultimately were transferred for higher-level care within the same hospital or shock hub hospital, died in the hospital, or deteriorated to a higher shock stage. The median time to this primary endpoint was 16 hours, which presenter Saraschandra Vallabhajosyula, MD (Brown University, Providence, RI), described as being relatively faster than would be expected for patients in a low category of shock.
“Those with poor outcome often lingered in SCAI B shock much longer—a median duration of 11 hours—as compared to 5 hours in those who had a favorable outcome, which was no escalation of SCAI stage, no escalation to a higher level of care, and survival of the hospitalization,” he added.
In a press conference prior to his presentation, Vallabhajosyula said better cardiogenic shock education across disciplines, including emergency department staff and emergency medical services personnel who encounter these patients first, is important to improving outcomes.
“Number two is developing smart EMR-based detection tools that will alert the provider,” he said. Often referred to as “sniffers,” these automatic alert systems, which are already in use for sepsis detection, could potentially be crafted to address early cardiogenic shock detection. An early sniffer, he added, “can then morph into clinical decision support systems that [walk the clinician through] meeting parameters and then use that as a scaffold for launching the shock team.”
Hypotension and AKI Portend Poor Outcomes
Vallabhajosyula and colleagues included patients (mean age 76 years; 43.8% women) admitted to the medical, intermediate care, and critical care units of six hospitals within the Brown University Health system between 2017 and 2022. The etiology of cardiogenic shock was heart failure in 42%, arrhythmia in 25%, acute MI in 13%, structural heart disease in 3%, and a combination of any of these factors in 17%. More than 40% of patients had stage II-V chronic kidney disease.
Hypoperfusion (blood lactate level of 2-5 mEq/L) was present in 83.2% of patients and hypotension (systolic BP ≤ 90 or mean arterial pressure ≤ 65 mm Hg) over two consecutive measurements in 16.8%. A higher percentage of those with hypoperfusion had a favorable outcome than those with hypotension (78.5% vs 51.7%).
In-hospital mortality rates were 15.4% in those with hypotension and 9.5% in those with hypoperfusion. Similarly, deterioration to a higher shock class occurred in 36.3% of those with hypotension and 11.8% of those with hypoperfusion, with rates of transfer for a higher level of care of 25.3% and 10.5%, respectively.
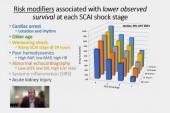
The most significant factors correlated to a poor outcome while in SCAI stage B were acute kidney injury (AKI), diuretic resistance, and oliguria in the prior 24 hours. In a multivariable analysis, AKI and a lack of diuretic response remained key predictors of poor outcome. Patients with AKI who had favorable outcomes tended to have earlier-stage AKI than those who had poor outcomes. Additionally, noninvasive positive pressure ventilation was higher at every time point in patients with poor outcomes versus those with favorable outcomes.
“These patients are telling us that they’re not doing well, and this potentially can be detected with routine vitals monitoring or even with increased frequency of monitoring,” Vallabhajosyula concluded.
He added that methods to improve delayed recognition and documentation of SCAI stage B should be a research priority and that the cardiorenal implications of early cardiogenic shock deserve further exploration.

L.A. McKeown is a Senior Medical Journalist for TCTMD, the Section Editor of CV Team Forum, and Senior Medical…
Read Full BioSources
Vallabhajosyula S. Etiology, management, and outcomes of SCAI stage B cardiogenic shock. Presented at: SCAI 2025. May 1, 2025. Washington, DC.
Disclosures
- Vallabhajosyula reports no relevant conflicts of interest.
Related News


Comments