AV Junction Ablation Plus CRT Cuts Deaths in Permanent AF Subset
The small trial supports the approach as first-line therapy in this group, particularly those with low EF, Michael Glikson says.

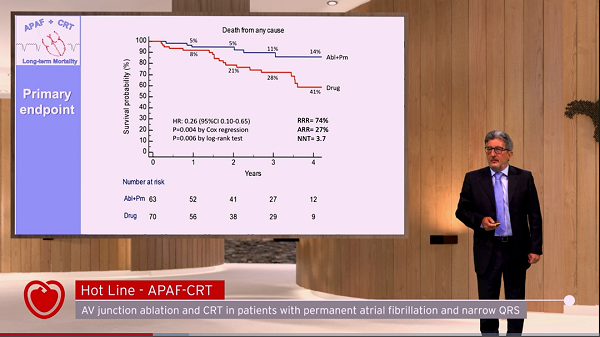
Atrioventricular (AV) junction ablation plus cardiac resynchronization therapy (CRT) reduces mortality in patients with symptomatic permanent atrial fibrillation (AF), a narrow QRS, and a recent heart failure (HF) hospitalization when compared with pharmacological rate control, the APAF-CRT trial shows.
Through a median follow-up of 29 months, 11% of patients randomized to ablation-CRT died from any cause, significantly lower than the 29% of patients who died after randomization to the trial’s drug therapy arm (HR 0.26; 95% CI 0.10-0.65), Michele Brignole, MD (Ospedali del Tigullio, Lavagna, Italy), reported at the virtual European Society of Cardiology (ESC) Congress 2021. The number need to treat was 3.7.
The findings were consistent regardless of whether baseline ejection fraction was above or below 35%, according to results that were published simultaneously online in the European Heart Journal.
“The benefit was due to the combination of the strict rate control and rate regularization achieved by AV junction ablation together with biventricular pacing, which counteracted the adverse effects of right ventricular pacing,” Brignole said, adding that the trial supports use of “ablation-CRT as a first-line therapy in patients with permanent AF and narrow QRS who were hospitalized for heart failure.”
The trial “makes an important contribution to establishment of AV nodal ablation with CRT as first-line therapy of resistant atrial fibrillation with [congestive heart failure], mostly in patients with reduced ejection fraction,” he commented. “The jury is still out regarding the advantage of CRT over RV apical pacing in AV nodal ablation patients with normal or near-normal ejection fraction, and the role of conduction-system pacing remains to be established.”
APAF-CRT
In the earlier APAF trial, Brignole’s group showed patients undergoing AV junction ablation for severely symptomatic permanent AF fared better when they also received CRT rather than RV apical pacing.
The APAF-CRT trial was therefore designed to test whether AV junction ablation plus CRT would be superior to pharmacological rate control in this same patient group. The trial included patients with severe symptomatic permanent AF who were unsuitable for AF ablation or in whom AF ablation had failed; a narrow QRS (110 ms or less); and at least one HF hospitalization in the previous year.
There were two phases of the trial, one looking at impacts on morbidity and the other at effects on mortality. The morbidity results were published in 2018, showing that ablation-CRT reduced the primary composite outcome of death or hospitalization due to HF or worsening HF and also improved quality of life.
The investigators kept enrolling patients for the mortality phase, reaching an enrollment of 133 patients (mean age 73 years; 47% women) when the trial was stopped prematurely at an interim analysis due to clear evidence of benefit. Heart rate was optimized at 30 days after randomization, coming in at 70 bpm in the ablation-CRT arm and 82 bpm in the drug arm.
Estimated mortality rates began to separate between the ablation-CRT and drug groups by 1 year (5% vs 8%), with the gap widening at 2 years (5% vs 21%), 3 years (11% vs 28%), and 4 years (14% vs 41%).
The advantage for ablation-CRT was similar in patients with an ejection fraction of 35% or less (HR 0.34) and in those with a higher EF (HR 0.27).
The secondary endpoint of all-cause mortality or HF hospitalization also was significantly lower in the ablation-CRT arm (29% vs 51%; HR 0.40; 95% CI 0.22-0.73).
A Relatively Common Problem
Glikson said “the results are not surprising. They are in line with the prior studies with shorter follow-up, and they justify a relatively common practice today to implant CRT in these patients.”
It’s unclear, he noted, how many patients had normal or near-normal EF and whether the trial results would apply to them. That’s an important issue, he explained, because when the new pacing/CRT guidelines were being developed, there was discussion about whether there’s an EF limit above which CRT is not needed following AV nodal ablation. The guideline writers decided to recommend CRT as the first choice in patients who have an indication for AV nodal ablation and a low EF, whereas in patients with normal EF, RV apical pacing was given a stronger recommendation than CRT (class IIa versus class IIb).
Thus, APAF-CRT “does not really change this approach presented here because we don’t have enough information on patients with normal or near-normal ejection fraction who are undergoing AV nodal ablation,” Glikson said.
Commenting for TCTMD, Joseph Marine, MD (Johns Hopkins Medicine, Baltimore, MD), chair of the American College of Cardiology’s Board of Governors, said the approach employed in APAF-CRT is currently being done in practice in patients with HF and AF, although it’s generally performed in patients with faster heart rates and only after pharmacological rate control and other treatments have failed.
“But this suggests that in some selected patients, completely controlling their ventricular rate with AV node ablation and biventricular pacing may be beneficial,” he said.
The small size of the study needs to be considered when interpreting the mortality difference observed between groups, Marine said. He noted that HF and AF frequently occur together, indicating that the trial population was a highly selected group of patients.
A larger trial would be needed to definitively prove a mortality benefit, he said. “However, in this group of patients, you often don’t have a lot of options for treatment to improve their quality of life.” The morbidity findings from APAF-CRT showed that ablation-CRT reduced symptoms and hospitalizations, which is “a benefit in and of itself,” so any improvement in mortality “is kind of icing on the cake,” Marine commented.
Ultimately, he said, “this is a therapy that can be considered in patients with advanced heart failure who have been hospitalized and are risk for rehospitalization despite optimal medical therapy for their heart failure if they have permanent atrial fibrillation that’s not amenable to attempts at rhythm control.”
But taking a broader perspective, Marine underscored that “the study also points to the importance of early treatment of atrial fibrillation, both with preventive therapies—weight loss, exercise, treatment of sleep apnea, risk factor reduction, etc—and [with] early rhythm control to prevent patients from getting to the situation where they need to have this therapy.”
Also at ESC 2021, in the same Hot Line session as APAF-CRT, results of the DECAAF II trial showed that image-guided fibrosis ablation added to pulmonary vein isolation (PVI) did not improve success rates compared with PVI alone among patients with persistent AF, although there were hints of benefit in patients with low levels of fibrotic disease in an as-treated analysis.

Todd Neale is the Associate News Editor for TCTMD and a Senior Medical Journalist. He got his start in journalism at …
Read Full BioSources
Brignole M, Pentimalli F, Palmisano P, et al. AV junction ablation and cardiac resynchronization for patients with permanent atrial fibrillation and narrow QRS: the APAF-CRT mortality trial. Eur Heart J. 2021;Epub ahead of print.
Disclosures
- APAF-CRT trial is an investigator-initiated, independent clinical trial, sponsored by a nonprofit organization called Centro Prevenzione Malattie Cardiorespiratorie ‘Nuccia e Vittore Corbella’, Rapallo, Italy, which received an unrestricted research grant from the Boston Scientific Investigator Sponsored Research (ISR) Committee.
- Brignole reports no relevant conflicts of interest.
- Glikson reports travel/meeting support from Boston Scientific and Sorin Group; and institutional research funding from Biotronik, Medtronic, and Pfizer.
Related News


Comments