MitraClip Helps for Atrial Functional MR: MITRA-TUNE
In patients with preserved LV function and/or AF, edge-to-edge repair leads to improved MR grade and symptom relief.


PARIS, France—Patients with atrial functional mitral regurgitation (MR) appear to benefit from edge-to-edge leaflet repair, data from the MITRA-TUNE registry suggest.
In patients with mitral regurgitation stemming from left atrial enlargement with atrial fibrillation (AF) but with preserved LV function and no leaflet degeneration, MitraClip (Abbott) repair led to significant improvement in their MR status and symptoms, as well as positive remodeling of the left atrium and mitral annulus.
Antonio Popolo Rubbio, MD (IRCCS Policlinico San Donato, Milan, Italy), who presented the results of MITRA-TUNE during a late-breaking clinical update at EuroPCR 2022, explained that atrial functional MR differs from classic functional MR in that it occurs in patients with AF and/or heart failure with preserved ejection fraction (HFpEF).
“It’s a newer subtype of secondary mitral regurgitation that has been introduced in the last 10 years,” Rubbio told TCTMD. In this case, he said, patients have normal systolic left ventricular function and normal leaflet motion. In AF, though, the left atrium can become stiff and fibrotic, which can cause severe dilatation of the left atrium. This results in dilation of the mitral annulus and impaired annular contractility.
Even in the absence of AF, however, HFpEF can result in atrial functional MR. “It’s like a vicious cycle in which we have preserved ejection fraction, left atrium dilatation with increased left atrium pressure that can cause the electrical disorders,” said Rubbio.
The prevalence of atrial functional MR is unknown, he added, although it’s thought to range between 3% and 15%. It is associated with a higher risk of adverse outcomes compared with AF patients without functional MR, but current guidelines do not provide any recommendations on how to best treat it, which is problematic in elderly patients.
“We have surgical treatment for younger people, or for those with fewer comorbidities,” said Rubbio. “In this case, we’re talking about an elderly cohort who weren’t eligible for surgery.” While mitral regurgitation can be influenced by medical therapy, these patients have HFpEF for which pharmacologic treatment is extremely limited, he said. “It’s not so easy to give medical therapy. Most of these patients were treated with beta-blockers because of their arrhythmia but beta-blockers are not the main treatment in preserved ejection fraction.”
MITRA-TUNE Follow-up in a Small Cohort
For the MITRA-TUNE study, investigators retrospectively reviewed 1,135 symptomatic patients with more than moderate functional MR who underwent transcatheter mitral valve repair with MitraClip in seven Italian centers. The analysis focused solely on 87 patients (median age 81 years) with mostly persistent/permanent AF and functional MR without structural leaflet abnormalities and preserved left ventricular function. Prior to the procedure, two-thirds of patients had MR grade 4+ while 83% of patients had NYHA class III/IV symptoms.
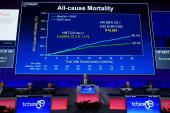
At 30 days, the cumulative risk of all-cause mortality was 5.0%. After a median follow-up of 371 days, the vast majority of patients had an improvement in MR—47 of 53 patients with available echo data had an MR grade ≤ 2+. Similarly, for the 61 patients with data, 48 (79%) were now in NYHA class I/II after a median follow-up of 489 days. Echo analysis of the left atrium and mitral annulus also showed that use of the MitraClip was associated with significant positive remodeling. In a multivariable analysis, postprocedural MR grade ≥ 2+ and a mitral annular diameter > 35 mm were both independent predictors of all-cause mortality/HF hospitalization.
To TCTMD, Rubbio said the study has limitations, noting foremost that it is a retrospective analysis. In terms of future research, he said it will be important to understand how patients respond to MitraClip in addition to the restoration of normal sinus rhythm, such as after catheter ablation of AF. In addition, they will need to understand more about managing pharmacotherapy for these patients, not only with beta-blockers but also with oral anticoagulation.
Ulrich Schäfer, MD (Marienkrankenhaus Hamburg, Germany), one of the panelists during the late-breaking clinical trials session, said that atrial functional MR appears to be a good indication for edge-to-edge repair with MitraClip, noting that the phenotype is clearly an “annular disease problem” given that larger mitral annular diameters were independent predictors of worse outcomes.
Rubbio noted that while the outcomes suggest edge-to-edge repair could be an option for elderly patients unable to undergo surgery, the results could still be improved. With MitraClip, previous studies have shown that the most-favorable results are seen in patients with residual MR grade 1+. The introduction of newer-generation MitraClip devices should help operators achieve better outcomes, he said.
“We know that it’s an important difference,” said Rubbio. “Moderate residual mitral regurgitation is considered a negative predictor of outcomes when compared with mild mitral regurgitation. An acceptable result is not the same as an optimal result.”

Michael O’Riordan is the Managing Editor for TCTMD. He completed his undergraduate degrees at Queen’s University in Kingston, ON, and…
Read Full BioSources
Rubbio AP, Testa L, Grasso C, et al. MitraClip in atrial function mitral regurgitation: a multicenter experience. Presented at: EuroPCR 2022. May 19, 2022. Paris, France.
Disclosures
- Rubbio reports no relevant conflicts of interest.
Related News


Comments