SGLT2i May Be Helpful Early After Acute MI in Diabetic Patients
The observational results are hypothesis-generating, but more-definitive randomized trial data are coming soon.


Early use of sodium-glucose cotransporter 2 (SGLT2) inhibitors may improve outcomes among patients with type 2 diabetes undergoing PCI for an acute MI, a retrospective study indicates.
Those started on an SGLT2 inhibitor within 2 weeks had a lower risk of all-cause mortality or hospitalization for heart failure (HF) through about 2 years of follow-up (9.8% vs 13.9%), as well as lower risks of each component of that composite endpoint and of MACE (all-cause death, nonfatal MI, or nonfatal ischemic stroke).
“Taken together with the proven cardioprotective effects of sodium-glucose cotransporter 2 inhibitors, our results suggest that the use of [the drugs] could expand to the acute phase of acute myocardial infarction survivors with diabetes to reduce mortality and the subsequent development of congestive heart failure,” researchers led by Osung Kwon, MD, PhD (Eunpyeong St. Mary’s Hospital, Seoul, South Korea), and Jun-Pyo Myong, MD, PhD (Seoul St. Mary’s Hospital), write.
Additional studies, including randomized controlled trials with long-term follow-up, are warranted to evaluate the impact of SGLT2 inhibition after acute MI, they add.
The study was published online recently in the Journal of the American Heart Association.
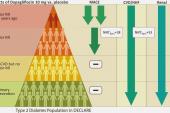
SGLT2 inhibitors, initially developed as antihyperglycemic agents, have been shown to reduce the risk of HF hospitalization in patients with type 2 diabetes who have or are at risk for CVD, and in a subanalysis of the DECLARE-TIMI 58 trial, dapagliflozin (Farxiga; AstraZeneca) reduced both MACE and CV death/hospitalization for HF in the subset of patients with a history of prior MI.
More recently, the medications have proven themselves in large trials of patients with chronic HF, regardless of diabetes status, although these excluded patients with a recent MI. So there remains a question about the impact of SGLT2 inhibitors in that scenario.
Early After MI
To address the question, Kwon, Myong, and colleagues examined claims data from the National Health Insurance Service of South Korea. Out of 30,635 patients with type 2 diabetes who underwent PCI for a first-time acute MI between January 2014 and August 2018, they matched 938 who started an SGLT2 inhibitor within 14 days with 1,876 who did not based on a propensity score. After matching, the mean age was 57.2, and 80% of patients were men.
The most common SGLT2 inhibitor was dapagliflozin (64.5%), with 32.2% started on empagliflozin (Jardiance; Boehringer Ingelheim/Eli Lilly) and 3.3% started on ipragliflozin.
The primary endpoint was a composite of all-cause mortality and hospitalization for HF, and this was a relative 32% less likely among patients treated with an SGLT2 inhibitor through a median follow-up of 2.1 years (adjusted HR 0.68; 95% CI 0.54-0.87). Risk of MACE, a secondary endpoint, was a relative 23% lower (adjusted HR 0.77; 95% CI 0.60-0.99).
Use of an SGLT2 inhibitor was associated with lower risks of both all-cause mortality (3.7% vs 6.6%; P = 0.002) and hospitalization for HF (7.4% vs 9.8%; P = 0.03), although there were no differences in nonfatal MI or ischemic stroke.
Awaiting the Randomized Trials
Smaller trials have tested the use of SGLT2 inhibitors in more-acute settings. Empagliflozin had beneficial effects in the 530-patient EMPULSE trial of patients with acute de novo or decompensated chronic HF. In addition, the drug provided a greater reduction in NT-proBNP and improvements in echocardiographic measures in the 476-patient EMMY trial when started within 72 hours of PCI in patients with acute MI.
In the context of those results, Kwon et al write, “our results supported the likelihood that patients could derive benefit from in-hospital SGLT2 inhibitor initiation after acute MI. However, a prospective randomized clinical trial in an acute MI population is required to ascertain whether SGLT2 inhibitors reduce deaths, the development of HF, and atherothrombotic vascular events.”
The results of trials in acute MI are coming, with DAPA-MI in patients without known diabetes and EMPACT-MI in patients with or without diabetes at or nearing completion.
Speaking with TCTMD, Jacob Udell, MD, who wrote an accompanying editorial with Jairo Nunes, MD (both from the University of Toronto, Canada), also highlighted the need for more-definitive data, noting that—at least in the realm of HF—there has been a push to get SGLT2 inhibitors started early on. “We've seen it work in heart failure. Why not in MI?” he said.
There are limitations with an analysis like the current one, Udell highlighted, pointing in particular to issues regarding selection of a comparator. “The dirty little secret is it's very hard to find a control group which is a fair comparison that doesn't have baked-in potential risk of confounding,” he said.
That’s why there is a need for caution when interpreting retrospective analyses like this one, he indicated. “There may be a survival bias that would allow for there to look like there's an association with protection, because the patients who are ultimately deemed to be on the trajectory of doing well are going to be the ones that get these therapies before the ones who look very brittle, very unstable, and we're going to hesitate to give those medicines,” he explained. “And then it looks like it's the medicine that did it, but it's really the company that it keeps that is associated with the good outcome.”
The dirty little secret is it's very hard to find a control group which is a fair comparison that doesn't have baked-in potential risk of confounding. Jacob Udell
He pointed out, too, that the patients who received SGLT2 inhibitors early after acute MI accounted for only 3.3% of the total potential cohort of patients undergoing PCI.
“This isn't a very representative sample of the general population showing up with type 2 diabetes and MI, and as a result, there may have been something particularly special or promising about these patients for which they started these therapies,” Udell said.
Even so, the findings are “very exciting” and raise questions about whether physicians should be acting on this information, he said. He cautioned, however, that this is a “great hypothesis-generating question and it's really important to answer this, I think, definitively in a randomized controlled trial.”
When DAPA-MI and EMPACT-MI report results, it will provide information on more than 10,000 patients combined after acute MI, Udell said, adding that he hopes the findings will come out in the next year.
“We'll see, hopefully, a signal and a significant benefit that will, I think . . . impact the standard of care,” he said. Together, he added, prospective trials and retrospective studies like this one will “hopefully open the stage for a paradigm shift in MI care.”

Todd Neale is the Associate News Editor for TCTMD and a Senior Medical Journalist. He got his start in journalism at …
Read Full BioSources
Kwon O, Myong J-P, Lee Y, et al. Sodium-glucose cotransporter-2 inhibitors after acute myocardial infarction in patients with type 2 diabetes: a population-based investigation. J Am Heart Assoc. 2023;12:e027824.
Nunes JT, Udell JA. So much to say on the best of what’s around regarding sodium-glucose cotransporter-2 inhibitors in acute myocardial infarction. J Am Heart Assoc. 2023;12:e030495.
Disclosures
- The study was partly supported by The Research Institute of Medical Sciences, The Catholic University of Korea, Eunpyeong St. Mary’s Hospital.
- Kwon, Myong, and Nunes report no relevant conflicts of interest.
- Udell reports having served as a consultant or speaker for AstraZeneca, Bayer, Boehringer Ingelheim–Lilly, Janssen, Novavax, Novartis, and Sanofi and having received research grants from AstraZeneca, Amgen, Bayer, Boehringer Ingelheim–Lilly, and Janssen.
Related News


Comments