Sweet Spot for Omecamtiv Mecarbil in HFrEF May Lie in Low SBP Patients
An agent that improves cardiac function without impacting systolic BP would be a welcome addition, experts say.


MADRID, Spain—Omecamtiv mecarbil (Cytokinetics) may be particularly useful for patients with heart failure and reduced ejection fraction (HFrEF) accompanied by low systolic blood pressure (SBP), according to new data from GALACTIC-HF.
As noted by Marco Metra, MD (University of Brescia, Italy), who presented the analysis here at the European Society of Cardiology 2022 Heart Failure congress, this particular patient group “remains a major challenge.”
“Low systolic blood pressure identifies patients with HFrEF at increased risk of clinical events, who poorly tolerate guideline-directed medical therapy,” he said. Moreover, “these patients are typically excluded from HFrEF trials due to the hypotensive effects of many therapies for HFrEF.”
The hope, he said, is that omecamtiv mecarbil, which directly improves cardiac contractility and function without reducing blood pressure, might be especially helpful in these patients.
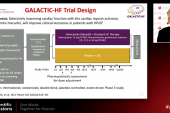
As previously reported by TCTMD, the main GALACTIC-HF results, reported back in 2020, showed that omecamtiv mecarbil, a novel selective cardiac myosin activator, significantly reduced rates of HF events or CV death: an absolute reduction of 2.1% and a relative reduction of 8% over a median follow-up of about 22 months. Discussion following the presentation of those primary results turned to the question of where this drug might fit given the relatively modest effect of the agent, particularly as compared with the impact of the range of medications now available for HFrEF patients.
The US Food and Drug Administration is currently reviewing the new drug application for omecamtiv mecarbil, with a deadline of November 30, 2022, to render its decision.
Low SBP Group Benefits
Of the 8,232 patients enrolled in GALACTIC-HF, 1,473 patients had SBP levels ≤ 100 mm Hg. Compared with patients with SBP > 100 mm Hg, the low SBP patients had lower rates of diabetes and hypertension and slightly lower LVEFs, but they were more likely to be seen in the inpatient setting and more likely to have an HF etiology other than ischemic heart disease.
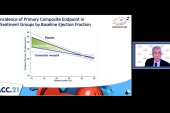
Adjusted for a range of patient characteristics and comorbidities, hazard ratios per 5-mm Hg decrease showed that patients at the lower end of SBP were significantly more likely to see a benefit of omecamtiv mecarbil as compared with placebo, a difference that diminished as SBP levels climbed. This held true for the primary endpoint of CV death or first heart failure event combined, for first heart failure events, and for CV death.
Using an SBP of 100 mm Hg as the cut point, patients with low SBP treated with omecamtiv mecarbil compared to placebo had significant reductions in the primary endpoint over a 36-month period, with curves separating in the first 6 months (although the number of patients available for follow-up declined markedly as time went on). These changes amounted to an absolute risk reduction of 9.8 events per 100 patient-years and a relative risk reduction of 0.81 (95% CI 0.70 to 0.94), Metra said.
By contrast, Kaplan-Meier curves for the primary endpoint in patients with SBP over 100 mm Hg were nearly superimposable for the omecamtiv mecarbil and placebo groups over 3 years of follow-up.
As expected, no significant impact of the drug on blood pressure was noted.
Welcome News
Following Metra’s presentation, session moderator John Cleland, MD (University of Glasgow, Scotland), called SBP a “biologically plausible biomarker,” noting “we need more treatments for patients who have borderline renal function and hypotension where many of our treatments are contraindicated or have to be used cautiously, so I think this is really welcome.”
Anu Lala, MD (Icahn School of Medicine at Mount Sinai, New York, NY), commenting on the analysis for TCTMD, agreed, calling the data “quite compelling.”
“Many of us who care for patients with advanced heart failure were eager to see these data,” she said in an email, noting that this subanalysis “gets at a sicker population” that included more inpatients, more patients with NYHA class IV symptoms, high NT-proBNP levels, more impaired renal function, and more CRT/ICD implantations.
“Patients who fit such a clinical profile can prove challenging to treat in that they may not tolerate target doses of guideline-directed medical therapy, but also may not quite be at the point to derive benefit from advanced therapies,” Lala said. “Yet they remain at high risk of adverse outcomes.”
As such, the nearly 20% relative risk reduction in CV death/first HF event is “encouraging,” Lala continued. Questions of cost and access still need to be answered, as will those related to the efficacy of omecamtiv mecarbil on top of sodium-glucose cotransporter 2 (SGLT2) inhibitors, which tend to have less of an adverse impact on blood pressure and were used in just 3% of GALACTIC-HF patients, she noted.
“I also look forward to learning the impact on patient-centered outcomes and would continue to recommend the referral of such patients to heart failure specialists for further risk stratification as to appropriateness for consideration of advanced therapies, including mechanical circulatory support and transplantation,” she said.

Shelley Wood was the Editor-in-Chief of TCTMD and the Editorial Director at the Cardiovascular Research Foundation (CRF) from October 2015…
Read Full BioSources
Metra M. Effects of omecamtiv mecarbil in patients with HFrEF and low blood pressure: results from GALACTIC-HF. Presented at: ESC-HF 2022. May 21, 2022. Madrid, Spain.
Disclosures
- Metra reports receiving personal honoraria and funding to his institution from Amgen and Cytokinetics as a participant to the Executive Committee and for patient enrollment in this trial; consulting fees for participation in advisory boards from AstraZeneca, Bayer, and Boehringer Ingelheim; personal fees as a member of executive or data monitoring committees of sponsored clinical trials from LivaNova and Vifor Pharma; and speaker fees from Abbott Vascular and Edwards Lifesciences. He has also participated on data safety and monitoring boards for Actelion.
- Lala reports receiving speaker fees from Novartis and Zoll and serving on advisory boards for Bioventrix and Merck.
Related News

Comments