Dapagliflozin US Cost-effectiveness Data Expose Barriers to HF Care
US costs for the drug are higher than in other countries, where studies have shown better cost-effectiveness ratios.


Adding dapagliflozin to standard heart failure therapies provides “intermediate value” for American patients who have heart failure with reduced ejection fraction (HFrEF), a new cost-effectiveness analysis suggests—at odds with earlier analyses that suggested the cost per quality-adjusted life-year (QALY) would be below the accepted $50,000 cutoff.
That’s because earlier studies, focused on settings outside the United States, considered both the “markedly lower” costs of the drug in countries like the United Kingdom, Germany, and Spain, as well as the lower overall healthcare costs in those nations, investigators led by Justin Parizo, MD (Stanford University, CA), say.
“Cost-effectiveness analyses are inherently tied to the society in which they’re evaluated,” senior author Alexander Sandhu, MD (Stanford University), explained to TCTMD. “While the clinical benefits might be quite similar across different contexts and populations, the costs of therapy and the costs of chronic care can vary substantially, so in order to be relevant to a decision maker in a given country, that context and those costs have to be taken into account. That's why it’s important to have country-specific cost-effectiveness estimates of therapy, specifically to help healthcare systems and payers understand relative value and the need for investment in important therapies like dapagliflozin.”
First developed as a diabetes drug, dapagliflozin (Farxiga; AstraZeneca), a sodium-glucose cotransporter 2 (SGLT2) inhibitor, has since been approved by the US Food and Drug Administration as a HFrEF drug. Professional societies increasingly recommend a simultaneous “four-pillar” approach to initiating HF care, with an SGLT2 inhibitor joining an angiotensin receptor-neprilysin inhibitor (ARNI), beta-blocker, and mineralocorticoid receptor antagonist at the outset of care. As with the ARNI sacubitril/valsartan (Entresto; Novartis) before it, however, uptake of the SGLT2-inhibitor drug class has been slow, leading some to question the high costs and overall cost-effectiveness.
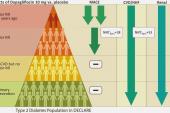
For their analysis, Parizo and colleagues used a Markov model to compare costs and outcomes between dapagliflozin and the standard of care across the pivotal DAPA-HF trial population. The price for the SGLT2 inhibitor in the model was pegged at $470 per month based on Centers for Disease Control and Prevention prescriber data.
Dapagliflozin provided a mean 0.78 more life-years and 0.46 additional QALYs compared with standard of care at an incremental cost of $38,212, for an overall cost per QALY of $83,650. That puts the therapy at “intermediate” value according to the accepted American College of Cardiology/American Heart Association benchmarks. The price of the drug would have to be cut by 43% (to $270 per month) in order to fall below the $50,000 cut point, at which therapies are deemed to be high value. Of note, the cost per QALY was similar for patients with or without diabetes as well as for those with mild or moderate cardiac impairment (with insufficient data for patients in NYHA class IV).
Barriers to Medications
To TCTMD, Sandhu stressed that cost is only one factor limiting uptake of these agents. He pointed to a recent CHAMP-HF registry analysis that detailed the factors associated with underprescribing and underdosing, even with relatively inexpensive heart failure medications.
“There are huge gaps in implementation for very low-cost, widely available therapies like mineral corticoid receptor antagonists,” Sandhu said. “But then you see that even amongst the therapies you can get at Target or Walmart for $4, we still have patients on inadequate doses of beta-blockers and ACE inhibitors or angiotensin receptor blockers or ARNIs.”
In addition to prohibitive pricing, Sandhu believes medication underuse can also stem from clinical knowledge gaps across the spectrum of physicians caring for heart failure patients. Or it can arise from clinician inertia when it comes to patients who are “stable” on their meds, “even though we see over and over again in these trials that the estimated risk reductions on a relative basis are just as large, if not larger, amongst the patients with milder heart failure,” he said. Patient inertia, too, is a hurdle, particularly if patients don’t feel their disease is adversely affecting their day-to-day lives.
The cost-sharing can still be too high, even with a $4 co-pay, for people that are clearly living on the borders of poverty or who have to decide between whether to pay for lifesaving therapies or to pay for their housing and food. Alexander Sandhu
Nevertheless, Sandhu continued, “I do think that cost and prior authorization are incredible barriers for patients, especially when it comes to the marked disparities we see across cardiovascular health.” Both in the outpatient and inpatient settings, the challenges to getting prior authorization are substantial. “And even when a therapy is approved by an insurer, the out-of-pocket costs are often prohibitive for patients,” he noted.
While there are financial assistance programs to help cover the costs of medications available to lower-income patients, too often these aren’t even used. “Unfortunately, the majority of patients who qualify for those programs are not enrolled,” Sandhu observed. “So increasing education and enrollment in those programs . . . are a step in the right direction, but for our most-vulnerable patients it’s still not enough. The cost-sharing can still be too high, even with a $4 co-pay, for people that are clearly living on the borders of poverty or who have to decide between whether to pay for lifesaving therapies or to pay for their housing and food.”
For all these reasons, said Sandhu, cost-sharing and co-pays don’t make sense.
“I think once we have therapies that are cost-effective and highly clinically effective, there shouldn't be cost-sharing; it's not what cost-sharing was designed for and it's quite counterintuitive that you'd want patient pharmaceutical cost-sharing for cost-effective, highly clinically effective therapies,” he argued. Hopefully, yes, drug costs will come down, particularly with more than one agent in the SGLT2 inhibitor class on the market. But cost-effectiveness analyses like this one, “hopefully push payers to be more inclusive about these therapies on their formularies and to lower barriers for patients getting on them,” Sandhu commented.
Unrealistic Expectations
In an accompanying editorial Derek Chew, MD, and Daniel Mark, MD (both from Duke Clinical Research Institute, Durham, NC), point out that a common misconception among heart failure physicians is that an effective therapy should also be “close to cost neutral, if not cost saving.”
In fact, they continue, as the dapagliflozin example makes clear, “the scenario of better outcomes for lower cost is unfortunately rare, with almost all new cardiovascular therapies increasing net costs.”
They estimate that out of the more than 3 million HFrEF patients in the United States, approximately 67% are expected to be candidates for an SGLT2 inhibitor. If all were to get the drug at its current price, the annual cost to society would be increased by a staggering $12 billion. While the “four-pillar” approach is advocated as the standard of care, they conclude, the affordability of such a strategy is unclear.
With agents like vericiguat (Verquovo; Merck) and omecamtiv mecarbil (Cytokinetics) progressing through positive trials, clinicians and patients face the likelihood that additional—and expensive—“pillars” may be recommended down the line, write Mark and Chew.
But even a four-pillar therapy “is aspirational at this point: what we think would be medically ideal in a world without the limitations imposed by the need to pay significant dollars for medical care,” Mark told TCTMD in an email. “The patchwork healthcare funding system in the US, together with the absence of any health-system-wide constraints on price/cost means that what is actually possible/affordable in the US now is going to vary enormously across patients. And in countries where the government health authorities play a more-proactive role in pricing/access, prices are much lower than in US.”
The slow uptake of dapagliflozin, and the role played by costs, is only exacerbating the situation seen with sacubitril/valsartan. “So far, available evidence suggest we are far underperforming in terms of use of sacubitril/valsartan relative to what the randomized controlled trial evidence would support and price/affordability/budget impact may be an important part of that story,” Mark noted. “Adding dapa introduces a 2X factor to the cost problem since it has about same price as Entresto.”

Shelley Wood was the Editor-in-Chief of TCTMD and the Editorial Director at the Cardiovascular Research Foundation (CRF) from October 2015…
Read Full BioSources
Parizo JT, Goldhaber-Fiebert JD, Salomon JA, et al. Cost-effectiveness of dapagliflozin for treatment of patients with heart failure with reduced ejection fraction. JAMA Cardiol. 2021;Epub ahead of print.
Chew DS, Mark DB. Dapagliflozin—Does Cost Make 4-Pillar Heart Failure Therapy Too Herculean a Labor for Medicine? JAMA Cardiol. 2021;Epub ahead of print.
Disclosures
- Parizo and Sandhu report no relevant conflicts of interest.
- Mark reports receiving grants from Merck, HeartFlow, and the Mayo Clinic outside the submitted work.
Related News


Comments