DISRUPT PAD III: Lithotripsy Prep Linked to Better PAD Patency at 1 Year
Adoption of IVL in the PAD space is likely to mirror the swift uptake seen in the coronaries, one panelist noted.

ATLANTA, GA—Intravascular lithotripsy (IVL) as a vessel-preparation technique prior to drug-coated balloon (DCB) therapy or stenting, compared with percutaneous transluminal angioplasty (PTA) alone, shows good patency to 1 year in patients with heavily calcified PAD, new data from the DISRUPT PAD III trial show.
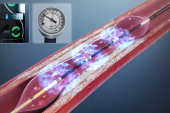
The findings provide insight into the mid-term benefits of the catheter-based delivery of acoustic pressure waves to crack large calcium deposits in the femoropopliteal arteries. Previously published reports from the DISRUPT PAD III investigators have demonstrated safety and procedural advantages of the technique in the short term.
In the latest report, which includes 306 patients with heavily calcified lesions, patency was greater at 1 year in the group treated with IVL (80.5% vs 68.0%; P = 0.017), senior researcher William A. Gray, MD (Main Line Health/Lankenau Heart Institute, Wynnewood, PA), said here at the Society for Cardiovascular Angiography and Interventions 2022 Scientific Sessions. Among a smaller group of patients with 2-year data, the patency results remained consistent, favoring IVL (74.4% vs. 57.7%; P = 0.005).
Interestingly, the patency rate in the PTA group is far better than would be expected at 1 year, something Gray said is likely the result of what the trial investigators told participating operators they wanted to see.
“We told all of them that the object of the study is for you not to fail,” he told TCTMD. “We wanted them to get to a lesion size of less than 30%, and they tried very hard to do that. “When they didn't do that, they put a stent in. So, there was aggressive vessel prep and then there was stenting, which confounded some of the patency analysis because stenting will add to patency.”
IVL slashed the overall need for stenting, however, with only one in 20 patients needing it compared with one in five in the PTA arm, he added.
Commenting in the session, panelist Gregg Stone, MD (Icahn School of Medicine at Mount Sinai, New York, NY), pointed out that despite the patency advantage, the IVL group showed no significant difference in clinical outcomes compared with PTA. Freedom from clinically driven TLR was 95.7% with IVL and 98.3% with PTA (P = 0.94), and the restenosis rate was 90.0% with IVL and 88.8% with PTA (P = 0.48).
In response, Gray noted that patient numbers are small, which limits definitive conclusion as to why a difference wasn’t seen, but maintained that not having a stent in place, especially in heavily calcified arteries, may offer the advantage of avoiding stent fractures that lead to restenosis over the long term.
DISRUPT PAD III Mid-term Results
The study, which was simultaneously published in Journal of the Society for Cardiovascular Angiography & Interventions, included PAD patients with moderate-to-severe calcification from 45 centers in the US, Germany, Austria, and New Zealand. Patients were randomized to vessel preparation with IVL (n = 153) or PTA (n = 153) followed by DCB and/or provisional stenting. Patient characteristics were similar in each treatment group, with the only difference being greater popliteal artery involvement in the IVL group (18.3% vs 9.8%; P = 0.03).
Procedural success was 65.8% in the IVL group and 50.4% of the PTA group. In addition to less provisional stenting, the IVL group also required less use of embolic protection and postdilatation, as well as lower maximum balloon inflation pressure.
In multivariable analyses, independent predictors of primary patency at 1 year were IVL, age > 75 years, and non-CTO lesions. Of the 35 patients in the study who received provisional stenting, restenosis occurred in two in the PTA arm and none in the IVL arm over the 2-year follow-up. A post hoc Kaplan-Meier analysis of the nonstented patients showed a similar pattern of better patency with IVL than with PTA at 2 years (78.6% vs 72.7%; P = 0.48).
Major adverse events occurred in none of the IVL patients and in 1.4% of PTA patients, for a P value of 0.15 at 1 year. There also were no between-group differences in ankle-brachial index, Walking Impairment Questionnaire, self-rated health scores, or Rutherford category from baseline to 1 year.
Quick Adoption Likely
Panelist Daniel M. Kolansky, MD (Hospital of the University of Pennsylvania, Philadelphia), noted that coronary operators have been responsible for a dramatic uptick in IVL in just over a year due to its ease of use. He suggested that the DISRUPT PAD III findings could contribute to a similar quick adoption of the device in the PAD space.
Gray agreed, adding that the device is faster and safer than atherectomy, which he said in his opinion isn’t even “a close second” as a management strategy for the type of heavily calcified peripheral lesions included in the trial.
In an editorial accompanying publication of the study results, Jennifer A. Rymer, MD (Duke Clinical Research Institute, Durham, NC), and colleagues agree these mid-term outcomes demonstrate that IVL should have “a significant role” in management of this patient population.
However, they note that more study is needed “to determine if there are types of calcified lesions where IVL is best utilized (ie, concentric vs eccentric), whether IVL has impact on drug uptake of the arterial wall, and in what clinical scenarios IVL should be considered vs atherectomy.”

L.A. McKeown is a Senior Medical Journalist for TCTMD, the Section Editor of CV Team Forum, and Senior Medical…
Read Full BioSources
Tepe G, Brodmann M, Bachinsky W, et al. Intravascular lithotripsy for peripheral artery calcification: 1-year and 2-year outcomes from the randomized Disrupt PAD III trial. JSCAI. 2022;Epub ahead of print.
Rymer JA, Armstrong E, Secemsky EA. Disrupting the management of calcified femoropopliteal peripheral artery disease: mid-term outcomes from Disrupt PAD III. JSCAI. 2022;Epub ahead of print.
Disclosures
- Gray reports consulting and institutional research support for Shockwave Medical.
- Rymer reports research support from Idorsia, Chiesi, Vascular Cures, and Women As One.
Related News


Comments