Enoxaparin Tops Aspirin for Preventing VTE After Hip or Knee Arthroplasty
The benefit in CRISTAL was driven by a lower rate of below-knee DVT, however, raising questions about clinical importance.


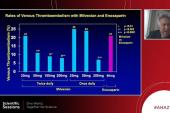
Aspirin alone doesn’t seem to be enough to prevent symptomatic venous thromboembolism (VTE) in the months following total hip or knee replacement for osteoarthritis, results of the CRISTAL trial indicate.
Designed to evaluate whether aspirin alone would be noninferior to enoxaparin, the trial—stopped early—ultimately demonstrated superiority for the low-molecular-weight heparin, which lowered the rate of symptomatic VTE through 90 days (1.82% vs 3.45%; P = 0.007), researchers led by Verinder Sidhu, MBBS (Hons), MS (UNSW Medicine and Health, Sydney, Australia), report.
The difference, however, was primarily driven by a reduction in below-knee deep vein thrombosis (DVT), an entity considered to be less clinically important than either above-knee DVT or pulmonary embolism (PE), which are more likely to be life-threatening. There were no significant differences between groups for those outcomes.
Thus, it’s unclear how the findings might impact everyday practice, which has seen increasing adoption of aspirin for thromboprophylaxis after joint replacement surgery in recent decades. That trend has been driven by supportive evidence from observational studies and randomized trials like EPCAT and EPCAT II, which demonstrated the noninferiority of using aspirin versus an anticoagulant after a brief period of anticoagulation, along with considerations around aspirin’s low cost, ease of use, and perceived lower risk of bleeding compared with the more-potent agents.
CRISTAL diverges from those prior trials in that patients in the aspirin arm did not first receive several days of anticoagulation before randomization.
“In the immediate post-op period, it may be that you need a higher-strength anticoagulant to prevent VTE but aspirin is [sufficient] for prolonged duration prophylaxis beyond that period,” Sidhu told TCTMD, adding that that’s the strategy he currently uses. He gives patients anticoagulation for at least the first 5 days after surgery and then evaluates risk factors like a prior history of VTE to decide whether to continue with anticoagulation or switch to aspirin.
The findings were published in the August 23/30, 2022, issue of JAMA.
The CRISTAL Trial
CRISTAL, performed across 31 hospitals in Australia that were doing more than 250 total hip or knee replacements each year, was a cluster-randomized, crossover trial nested within the Australian Orthopaedic Association National Joint Replacement Registry. Hospitals were randomized to first use aspirin or enoxaparin in adult patients undergoing total hip or knee arthroplasty before switching to the other treatment after enrollment targets were met for the initial assignment. About half of the hospitals crossed over to the other treatment before the end of the trial, which was prematurely halted after an interim analysis had determined the stopping rule was met.
Overall, 9,711 patients (median age 68 years; 56.8% women) were enrolled out of a planned 15,562. Among them, 58.4% received aspirin 100 mg/day after surgery and the rest received enoxaparin 40 mg/day. Treatment was continued for 35 days after hip replacement and 14 days after knee replacement.
The primary outcome was symptomatic VTE within 90 days, and the estimated difference in this endpoint between the aspirin and enoxaparin groups (1.97%; 95% CI 0.54%-3.41%) not only failed to meet the criterion for noninferiority at a margin of 1%, but also showed the superiority of enoxaparin. The component of the primary outcome that showed the greatest difference between groups was below-knee DVT, which occurred at double the rate in the aspirin arm (2.4% vs 1.2%; P = 0.004).
None of the secondary outcomes covering death, major bleeding, readmission, reoperation (at 90 days and 6 months), and drug adherence differed between groups.
Importance of Below-Knee DVT
The implications of the findings may hinge on how physicians interpret the importance of below-knee DVT, Sidhu indicated. Though it isn’t as dire as above-knee DVT or PE, he said, it’s still clinically relevant to prevent after joint replacement because it can cause pain and requires treatment with powerful anticoagulants, which in turn increases risks of secondary problems like bleeding from the surgical site and wound complications.
Considering CRISTAL in the context of the prior trials that randomized patients to aspirin only after several days of anticoagulation, Sidhu said it might be that aspirin doesn’t provide adequate protection in the days following surgery, a period when the thrombogenic risk is particularly high, but is sufficient later on.
If you could use a medication that reduces all VTE risk and doesn’t lead to an increased rate of mortality, bleeding, reoperation, or readmission, then I think we should probably use that medication over the other medication. Verinder Sidhu
Asked whether CRISTAL provides a definitive answer to the question of aspirin monotherapy’s utility in the immediate postoperative period, he said, “I think we have enough evidence in our patient population in Australia to suggest that aspirin is not sufficient for this purpose in the first 5 days after hip and knee replacement.” But some detractors might say that further trials powered specifically for above-knee DVT and PE are needed, Sidhu added, noting that there are other trials underway.
According to Noel Chan, MD (Population Health Research Institute, McMaster University, Hamilton, Canada), who wrote an accompanying editorial with Mohit Bhandari, MD, PhD (McMaster University), CRISTAL is an important step in the evaluation of aspirin as sole thromboprophylaxis after joint replacement.
And it comes in the context of a decades-long decline in rates of VTE in this setting and growing evidence of aspirin’s efficacy for primary and secondary VTE prevention, Chan told TCTMD, noting that aspirin has a low cost, has a perceived lower risk of bleeding, and is more convenient to use compared with anticoagulation. On that background, he said, the question of whether aspirin is noninferior to anticoagulation in terms of preventing symptomatic VTE has become more important.
When interpreting the findings, Chan raised issues about the relative importance of the various outcomes included in the primary composite endpoint, saying that PE sits at the top, followed by above-knee DVT and then below-knee DVT.
“I don’t think that . . . people who are using low-molecular-weight heparin are going to switch their practice, but at the same time, I don’t see people using aspirin [switching] their practice based on the clinical results, because the efficacy is mainly driven by an increase in below-knee DVT rather than any of the other outcomes that have been mentioned so far,” Chan said.
Guidelines list multiple potential thromboprophylaxis regimens after joint replacement, including low-molecular-weight heparin, direct oral anticoagulants, aspirin, or a hybrid of in-hospital anticoagulation followed by aspirin, but there remains a need for studies to help sort out which is best, Chan said, indicating that aspirin alone is still in the mix.
“There are a few changes that happened over the last few decades that are changing the epidemiology and the baseline rates [of VTE] that may make aspirin an attractive option in this particular setting,” he said.
For now, according to Sidhu, it might make sense to stick with what CRISTAL showed, which was a significantly lower rate of symptomatic VTE, including a nonsignificantly lower rate of PE, with enoxaparin versus aspirin. “If you could use a medication that reduces all VTE risk and doesn’t lead to an increased rate of mortality, bleeding, reoperation, or readmission, then I think we should probably use that medication over the other medication,” he said.

Todd Neale is the Associate News Editor for TCTMD and a Senior Medical Journalist. He got his start in journalism at …
Read Full BioSources
CRISTAL Study Group. Effect of aspirin vs enoxaparin on symptomatic venous thromboembolism in patients undergoing hip or knee arthroplasty: the CRISTAL randomized trial. JAMA. 2022;328(8):719-727.
Chan NC, Bhandari M. Thromboprophylaxis after hip or knee arthroplasty. JAMA. 2022;328(8):712-713.
Disclosures
- The study was funded by a 4-year Medical Research Futures Fund grant by the Australian federal government.
- Sidhu and Bhandari report no relevant conflicts of interest.
- Chan reports personal fees from Stago and Boehringer Ingelheim.
Related News


Comments