With Some Adjustments, Commissural Alignment Possible With TAVI
Aligning a THV with the native valve is critical as younger, low-risk patients are treated and future procedures are considered.


It is possible to safely achieve optimal commissural alignment of a self-expanding transcatheter heart valve (THV) in the majority of patients undergoing TAVI, a new study suggests. The implantation technique, which requires understanding how the native aortic valve commissures are situated in different fluoroscopic views, resulted in mild-or-less commissural misalignment in 88% of patients undergoing TAVI with a variety of valve types.
The modified approach, say investigators, is important because thinking about future procedures, such as redo TAVI or PCI, is increasingly relevant given the treatment of younger, lower-risk patients with aortic stenosis.
“Transcatheter valves have been implanted for more than 10 years now, but we’ve never paid much attention to commissural alignment,” study author Ole De Backer, MD, PhD (Rigshospitalet, Copenhagen University Hospital, Denmark), told TCTMD. “We were focused on sizing and how deep or high to implant the valves to prevent paravalvular leak and conduction disturbances. Of course, as we treat younger and younger patients, there are concerns about the need for coronary access because some of these patients will later present with ischemic heart disease where you’ll want to do a percutaneous coronary intervention.”
Gilbert Tang, MD, MBA (Mount Sinai Health System, New York, NY), who has investigated how to optimally align THVs with native aortic valve commissures, praised the investigators for their “provocative” study, saying it suggests it is possible to modify existing implantation techniques to optimize valve alignment. “It’s very elegant and nicely illustrated,” said Tang, “but it’s a small, proof-of-concept study that will require a larger number of patients to see if it can be broadly adaptable.”
The new study, as well as an accompanying editorial by Tang and Syed Zaid, MD (Houston Methodist DeBakey Heart and Vascular Center, TX), was published online September 15, 2021, ahead of print in JACC: Cardiovascular Interventions.
Problems When Commissures Don’t Align
With surgery, the bioprosthetic valve can be reliably aligned commissure-to-commissure with the native aortic valve, said De Backer, but THVs tend to land randomly with TAVI. With commissural misalignment, the commissural post blocks the coronary ostia, which in turn limits access for future interventions. However, commissural alignment with THVs would not only make coronary access possible but also be better for coronary blood flow, said De Backer. Additionally, bench testing suggests commissural misalignment might put undue stress on the THV leaflets, which raises concerns about valve durability.
“There is also good data out there that if you have commissural misalignment with your transcatheter heart valve, there is slightly more risk of mild leak,” said De Backer. “The orientation of the leaflets is important—nature made it in such a way that this is probably the best orientation for the best possible closure of the valve in diastole.”
Several researchers have attempted to modify the implantation of THVs to achieve better commissural alignment with the native aortic valve. This includes optimally deploying the valve in such a way so that it lands in alignment with native coronary anatomy.
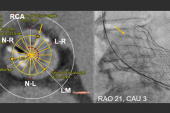
With this in mind, De Backer along with Gintautas Bieliauskas, MD (Rigshospitalet, Copenhagen University Hospital), and colleagues aimed to test a patient-specific method to obtain commissural alignment during implantation with three different self-expanding THVs: Evolut R/PRO (Medtronic), Acurate Neo2 (Boston Scientific), and Portico (Abbott). All patients underwent cardiac CT prior to TAVI, which allowed the operators to determine the patient-specific fluoroscopic projection in which the right and left coronary cusp overlap, the so-called RCC/LCC view. This projection, in combination with a prespecified orientation of the THV, was used to facilitate neo-commissural alignment.
“To be able to do an implantation with commissural alignment, you have to understand completely the commissural orientation in the different fluoroscopic views,” said De Backer. “When you understand how the commissures are oriented in the right and left cusp overlap view—that means you overlap the right and left coronary cusps on the right-hand side of your fluoroscopic screen—the commissure between these two cusps is facing to the right.”
The delivery system is inserted into the femoral artery based on THV type—flush port at 3 o’clock for Evolut, 6 o’clock for Acurate Neo2, and 12 o’clock for Portico. When the valve is deployed, the Evolut “Hat” marker is positioned in the center-front orientation while Acurate Neo2 and Portico are deployed with one of the commissural posts, which are visible under fluoroscopy, facing the right side of the fluoroscopic screen. The Evolut valve, at present, doesn’t have any markers that can be seen under fluoroscopy.
In their study, valve implantation was successful in all patients, with no damage to the delivery system and no procedural complications reported. In the post-TAVI assessment by CT, mild-or-less commissural misalignment (< 30°) was observed in 53 of 60 patients. Optimal alignment (< 15°) was obtained in 36 patients (60%). Severe misalignment (< 45°) with overlap between the coronary ostia and THV commissures, was seen in two patients. With the Acurate Neo2 valve, operators achieved the best success, with moderate-or-worse misalignment avoided in all cases.
Torquing Delivery Catheters, Ever So Slightly
To TCTMD, De Backer said that when they introduce the valves with a specific orientation, this only avoids a complete miss with the native commissures. Depending on patient anatomy, operators will attempt to achieve the best possible alignment by slowly torquing the delivery catheter when the valve is positioned in the aortic annulus. A flexible delivery catheter responsive to these minute rotations is important, said De Backer, adding that some catheters are easier to torque than others.
“To be honest, in most cases, in most patients, you can rotate enough to avoid absolute commissural misalignment,” said De Backer. “You can rotate enough to avoid the worst-case scenario and aim for an optimal alignment.”
To TCTMD, Tang said there are some questions remaining, such as whether the modified approach would be possible in patients with calcified and tortuous vessels. Additionally, he wondered about the torquing of the catheter—these “micro” adjustments to align the valve—and whether it is safe across a range of patients with different anatomies. The Portico and Acurate Neo2 delivery catheters, which are a little more flexible, might be better suited to the adjustments needed to achieve commissural alignment, he said.
“I can tell you, from my own personal experience, I wasn’t able to do that with the Evolut platform,” said Tang. “When you try to rotate the catheter, there is no translation at the annular level. I can’t speak for the Acurate and Portico—they are more flexible—but it is conceivable that once you cross the annulus you might be able to adjust orientation to optimize the alignment. Their sample size is small and needs to be validated in a larger study to confirm their findings. Still, this is a step in the right direction.”
In terms of reproducibility, the researchers say the implantation technique can be performed by all operators. In many of the large European TAVI centers, teams have already adopted the approach and are achieving good results, said De Backer. It’s not an implantation technique that’s difficult to learn, he said, though it does require some adaptation on the part of operators, such as learning how to optimally torque the delivery catheter to achieve good results.
De Backer said they opted to study the Acurate Neo2, Portico, and the Evolut valves because they are recapturable and repositionable, which was important in this study of commissural alignment. Tang, who previously reported that it was difficult to predict commissural alignment with the balloon-expandable Sapien valve, noted that the Sapien frame is shorter, which means coronary reaccess might be less of an issue, although it can still present problems in selected patient anatomies.

Michael O’Riordan is the Managing Editor for TCTMD. He completed his undergraduate degrees at Queen’s University in Kingston, ON, and…
Read Full BioSources
Bieliauskas G, Wong I, Bajoras V, et al. Patient-specific implantation technique to obtain neo-commissural alignment with self-expanding transcatheter aortic valves: results from the COMALIGN study. J Am Coll Cardiol Intv. 2021;Epub ahead of print.
Tang GHL, Zaid S. Commissural alignment using cusp-overlap view in self-expanding TAVR: a step closer to achieving surgical-like orientation? J Am Coll Cardiol Intv. 2021;Epub ahead of print.
Disclosures
- Tang reports serving as a physician proctor for Medtronic, consulting for NeoChord, consulting/serving on an advisory board for Abbott, and serving on an advisory board for Jena Valve.
- De Backer reports institutional research grants and consulting fees from Abbott and Boston Scientific.
Related News


Comments