Good News for Intravascular Imaging Continues at 5 Years: RENOVATE-COMPLEX-PCI
Final follow-up from the trial shows durable protection against TLF, especially in chronic total occlusions and diffuse long lesions.


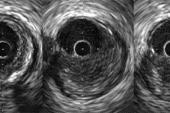
Intravascular imaging continues to provide better clinical outcomes for patients with complex coronary lesions at 5 years after PCI, according to new follow-up data from the RENOVATE-COMPLEX-PCI trial.
The trial’s previously reported main findings, with a median follow-up of 2.1 years, showed a relative 36% reduction in target-vessel failure—cardiac death, target-vessel MI, or clinically driven target-lesion revascularization—with intravascular imaging versus angiographic guidance. Target-vessel MI or cardiac death was reduced by 37%, and cardiac death alone by a 53%.
“What this 5-year report adds is durability,” Joo-Yong Hahn, MD, PhD (Samsung Medical Center, Seoul, Republic of Korea), the paper’s senior author, told TCTMD in an email. The earlier benefit has been “maintained over a median 5.3 years, without evidence of a late catch-up. In other words, the early procedural advantage translated into a sustained clinical benefit over time.”
This doesn’t come as a surprise but rather serves as a key confirmation that “when PCI is optimized properly at the index procedure, that benefit can persist for years in patients with complex coronary disease,” Hahn noted.
Still, despite growing evidence to support it, intravascular imaging has yet to be widely adopted in some regions, including the United States. Use has been on the upswing, however, thanks to its endorsement in the 2018 European and 2021 US revascularization guidelines. As of 2024 and 2025, respectively, European and US guidelines gave intravascular imaging a class 1a indication for guiding PCI in chronic and acute coronary syndromes.
“The main barriers are still cost, reimbursement, procedural time, and operator familiarity. Usage differs widely across the world because adoption depends not only on the evidence, but also on local healthcare systems, training environments, and device availability,” said Hahn, who predicted, “As the evidence and guideline support continue to strengthen, especially in complex PCI, I expect use of intravascular imaging to become more widespread.”
He advised that in contexts where such imaging can’t be routine, whether due to cost or some other barrier, “it should be prioritized for cases where it is most likely to alter procedural strategy or improve stent optimization.”
Led by Joo Myung Lee, MD, PhD (Samsung Medical Center), and Onyou Kim, MD (Samsung Medical Center and Korean University Anam Hospital, Seoul), the 5-year follow-up from RENOVATE-COMPLEX-PCI was published recently in JACC.
No Late Catch-up
For this analysis, follow-up was available at a median of 5.3 years for all 1,639 of the trial’s patients who had been randomized 2:1 to intravascular imaging or angiography guidance. Around half had initially presented with stable ischemic heart disease and half with acute coronary syndromes. The most common type of complex lesion was long coronary occlusion, followed by multivessel PCI, true bifurcation, and chronic total occlusion. More than three in 10 patients had at least three of the aforementioned characteristics in the target lesion.
The primary endpoint of TLF was significantly lower when intravascular imaging, compared with angiography, was used to guide PCI (10.5% vs 14.9%; HR 0.68; 95% CI 0.51-0.91). The composite of cardiac death or target-vessel MI occurred in 7.6% of the imaging group and 10.7% of the angiography group (HR 0.68; 95% CI 0.48-0.96). Clinically driven TLR rates were 4.4% and 6.2%, respectively, a nonsignificant difference (HR 0.73; 95% CI 0.46-1.16).
Landmark analyses showed that most of the advantage for intravascular imaging occurred within the first 2 years, with no significant difference between the two groups thereafter.
“Notably, within the spectrum of complex coronary artery lesion subsets, the benefits of intravascular imaging-guided PCI over angiography-guided PCI were most apparent in chronic total occlusion and diffuse long lesion[s],” the investigators point out. “Although there was no significant interaction between clinical presentation and treatment effect of intravascular imaging, patients with stable ischemic heart disease showed more prominent benefit . . . than those with acute coronary syndrome.”
[Intravascular imaging] should be prioritized for cases where it is most likely to alter procedural strategy or improve stent optimization. Joo-Yong Hahn
RENOVATE-COMPLEX-PCI stands out in the evidence base for the magnitude of improvement with intravascular imaging. “Prior studies of intravascular imaging-guided PCI have not always shown statistically significant reductions in hard endpoints, but the signal has generally been directionally consistent,” Hahn explained. “In RENOVATE-COMPLEX-PCI, the benefit may have been more apparent because the trial enrolled only complex lesions . . . where the impact of imaging is likely to be greatest, and because the longer follow-up allowed that benefit to become more evident over time.”
The reduction in cardiac death is consistent with results from a large meta-analysis presented at the 2023 European Society of Cardiology Congress, he observed. “Mechanistically, if imaging allows us to identify and correct underexpansion, malapposition, and edge complications at the index procedure, it reduces the substrate for later restenosis, stent failure, and thrombosis, which may ultimately translate into fewer myocardial infarctions and cardiac deaths.”
Hahn said that, with extended follow-up now reported, there likely are no more analyses from RENOVATE-COMPLEX-PCI on the way.
Instead, “I think the next step for the field is to better define how intravascular imaging should be integrated into contemporary PCI strategies,” he specified. “One study to watch is the ongoing FRAME-AMI2 trial, which is evaluating whether an intravascular imaging-guided PCI strategy is noninferior, and potentially superior, to a physiology-guided strategy for the treatment of nonculprit lesions in patients with acute myocardial infarction and multivessel disease.”

Caitlin E. Cox is Executive Editor of TCTMD and Associate Director, Editorial Content at the Cardiovascular Research Foundation. She produces the…
Read Full BioSources
Lee JM, Kim O, Song YB, et al. Intravascular imaging- vs angiography-guided complex PCI: 5-year outcomes from a randomized trial. JACC. 2026;Epub ahead of print.
Disclosures
- This trial is investigator-initiated with grant support from Abbott Vascular and Boston Scientific.
- Lee reports receiving institutional research grants from Abbott Vascular, Boston Scientific, Philips Volcano, Terumo Corporation, Zoll Medical, and Donga-ST.
- Kim reports no relevant conflicts of interest.
- Hahn reports receiving institutional research grants from Korea’s National Evidence-based Healthcare Collaborating Agency, Abbott Vascular, Biosensors, Boston Scientific, Daiichi Sankyo, Donga-ST, Hanmi Pharmaceutical, and Medtronic.
Related News

Comments